
by Matthew J. Zirwas, MD, and Jessica Moennich
Authors: Dr. Matthew J. Zirwas, MD, is Assistant Professor of Dermatology, The Ohio State University. Jessica Moennich is a Medical Student, The Ohio State University, Columbus, Ohio. The authors report no relevant conflicts of interest.
Case
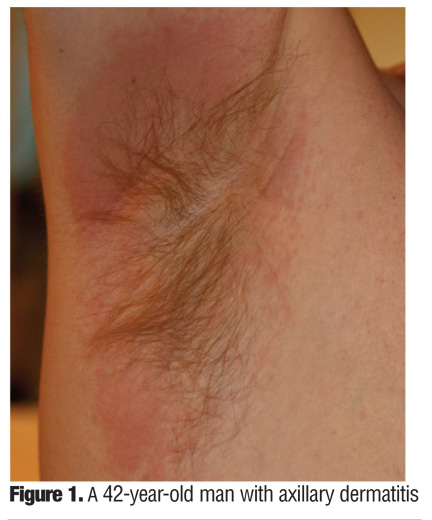
A 42-year-old man presented with a recurrent axillary dermatitis that had been ongoing for several years (Figure 1). The dermatitis was intensely itchy when present. He had been patch tested twice with the Thin-Layer Rapid Use Epicutaneous (T.R.U.E.) Test and no positive reactions had been found, leading to a diagnosis of irritant dermatitis and treatment with topical steroids on an as needed basis.
{kind=link}
Due to continued outbreaks, the patient referred himself to a contact dermatitis center where expanded patch testing was undertaken. He was found to have 1+ reactions to fragrance mix 1 and balsam of peru, and 2 to 3+ patch-test reactions to fragrance mix 2, compositae mix, ylang-ylang oil, lyral, tea tree oil, Arnica montana, lichen acid mix, and Lavender Absolute. He was patch-test negative to his current deodorant, but wished to use an antiperspirant/ deodorant combination product. Fragrance-free antiperspirant/ deodorant products were recommended and the patient’s eruption has not recurred.
Introduction
Deodorants and antiperspirants are two of the most commonly used cosmetic products, with millions of consumers applying these products to their axilla everyday. Deodorants are used to mask odor; whereas, antiperspirants are used to reduce the amount of sweat produced. These two activities are often combined into single products. While deodorants are considered cosmetic products because they do not change the function of the skin, antiperspirants are classified as drugs and are therefore subject to rules and regulations set forth by the Food and Drug Administration (FDA). The active ingredient in antiperspirants is usually aluminum based, which reduces sweat by causing obstruction of the eccrine glands.[1] Deodorants work by two different mechanisms—antimicrobial agents decrease the number of bacteria that produce volatile odoriferous substances and fragrances cover any odors that are produced.[1] Recently, naturally occurring zeolite minerals, in the form of potassium alum or ammonium alum crystals, have been marketed as all-natural alternatives to deodorants and antiperspirants. These products are sold in solid crystal form. The consumer is instructed to wet the crystal and apply the product to the underarm area to prevent odor. Although no research has been published evaluating the mechanism of action of these products, the company that markets them, Crystal Body Deodorant (French Transit, Ltd., Burlingame, California), claims that the mineral salts create an environment in which bacteria cannot survive.
Antiperspirants and deodorants are generally very safe products. However, these products have received much attention as the possible cause of increasing rates of breast cancer, with most hypotheses indicating the estrogenic properties of parabens as the main contributing factor. Numerous studies supporting[2] and discrediting[3] this claim have been published, but recently the FDA and the National Cancer Institute have stated that antiperspirants and deodorants are not linked to cancer. In addition to these concerns, aluminum exposure from deodorant use has been blamed for the rising incidence of Alzheimer’s Disease (AD). A recent review of 46 studies looking at aluminum exposure and risk of developing AD concluded that aluminum is, in fact, a risk factor for the development of disease.[4] However, this review evaluated oral, topical, and environmental exposure. There has been only one study specifically assessing the risk of developing AD with the use of aluminum-containing deodorants. This study looked at 130 matched pairs of cases and controls, and concluded that the odds ratio for the use of aluminum containing deodorants and the development of AD was 1.6, with higher risk associated with more frequent use.[5] However, these results were inconclusive due to the use of surrogate respondants and the length of time over which exposure may have occurred. Therefore, this topic remains controversial, although authors of the article review suggest that avoidance of general aluminum exposure may decrease the risk of developing AD.[4] Rare side effects from the use of antiperspirants and deodorants, such as the development of cutaneous granulomas,[6] have been reported, but the most frequently experienced adverse events are nonspecific irritant reactions and sensitization to compounds contained within the product resulting in the development of allergic contact dermatitis (ACD).
Cosmetic allergy is a common and frustrating problem. A recent survey in the United Kingdom found that 23 percent of female subjects and 13.8 percent of male subjects will experience an adverse reaction to a personal-care product in the course of a year.[7] Although not all of these reactions are allergic in nature, approximately 10 percent of patients patch tested will test positive for allergy to cosmetics.[7] Deodorants and antiperspirants are among the most common products causing cosmetic allergy, thus these products and their constituents are frequently used when patch testing individuals with ACD. In fact, in a review of patch-testing results from 1998 to 2002, the Information Network of Departments of Dermatology (IVDK) found that deodorants are the most frequently tested personal-care products.[8]
The axillary area may be predisposed to ACD, although this has not been conclusively demonstrated. Several factors may contribute to susceptibility to sensitization to products applied to the axilla, including differences in axillary skin phenotype9 and prolonged occlusion in the area.[10]
Following a positive patch test, finding deodorants or antiperspirants that are free of the detected allergens can be problematic for patients due to the widespread use of a number of common allergens. We sought to systematically evaluate the potentially allergenic ingredients in products that are widely available to consumers in the United States. This information should be helpful to clinicians who detect allergy to ingredients that are potentially present by allowing them to better assess the likelihood of past, present, and future exposure to these allergens via antiperspirants and deodorants.
Methods
We utilized a recently published database of all deodorants and antiperspirants available on the shelves at Walgreens Pharmacies (Chicago, Illinois).[11] For each product, this database lists all allergens from the North American Contact Dermatitis Group (NACDG) screening panel that are present. The information in the database was collected and extracted by a dermatologist with specific expertise in ACD. Using this database, we entered each deodorant or antiperspirant and the allergens in that product into a Microsoft Excel (Seattle, Washington) spreadsheet. Using filters, we then analyzed the number of deodorants or antiperspirants containing each allergen.
Results
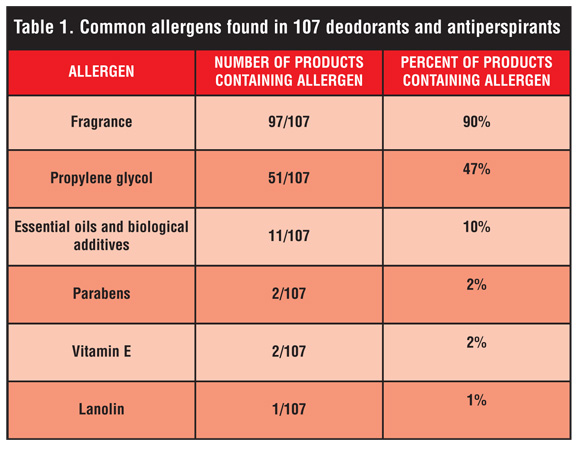
One hundred seven deodorants and antiperspirants were included in the database. Of the 107 products, 97 contained fragrance, making it the most commonly present allergen (Table 1). Of the 10 products that did not contain fragrance, two contained potential allergens that are fragrance related—essential oils and biological additives. Thus, there were eight products in the database that were truly fragrance free and definitely safe for patients with fragrance allergy.
{kind=link}
The second most commonly present allergen was propylene glycol (PG), a water-soluble vehicle ingredient, with 51 of the 107 deodorants or antiperspirants containing the solvent. The third most common allergens were essential oils and biological derivatives, which were found in 11 of the 107 products.
Parabens and Vitamin E (tochopherol) were each found in two of the 107 products. Parabens are frequently used preservatives, and vitamin E is commonly added to cosmetic products due to the belief that it has antioxidant properties. The final allergen found in the database was lanolin, which was present in one product.
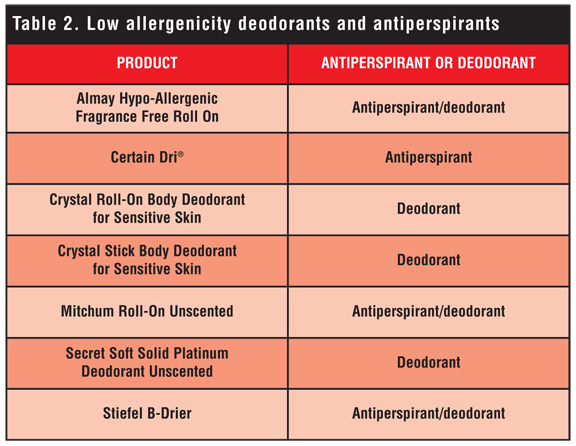
Several products are free of the most important allergens and can, therefore, often be empirically recommended in cases of suspected antiperspirant or deodorant allergy prior to patch testing. These products are listed in Table 2.
{kind=link}
Discussion
The most commonly occurring allergen found in our search was fragrance, which was present in 90 percent of the deodorants contained in the Walgreens database. Fragrance is added to deodorants not only to increase marketability, but also to enhance their function by counteracting underarm odor. Axillary dermatitis has been shown to be overrepresented in individuals with known fragrance allergies. In fact, history of a rash due to the use of a scented deodorant increases the risk of fragrance allergy by a factor of 2.4.[12] Also of note, a study performed by Johansen et al[13] demonstrated the ability of deodorants to elicit clinically significant allergic reactions in fragrance-sensitive individuals. In this study, which looked at 20 deodorants applied to the axilla and forearm of 14 patients, 60 percent of the deodorants tested resulted in a positive reaction, and the elicitation potential of each of these deodorants was related to the concentration of the allergen contained and not simply its presence in the product.[13] In general, ACD due to fragrance is a frequently encountered and frustrating clinical problem. Approximately 1 to 4 percent of the general population and 10 percent of the patch-test clinic population will experience ACD when exposed to fragrance.[11,14] This percentage is trending upward, possibly due to the increased use of fragrance-containing products.[15] About 3,000 compounds are used in the perfume industry, and individual products may contain anywhere from 10 to 300 of these,[16] making diagnosis and avoidance of the offending agent extremely difficult. Standard patch testing for fragrance allergy employs two allergens: fragrance mix and basalm of Peru. The most frequently encountered compounds responsible for ACD found in deodorants are geraniol, eugenol, and hydroxycitronellal, all of which are present in the fragrance mix.
Unfortunately, due to the evolving nature of the fragrances used by the perfume industry, the sensitivity of the fragrance mix and balsam of Peru is decreasing, and they are currently estimated to identify only 60 to 70 percent of individuals with fragrance allergy.[11] Therefore, when patients present with axillary dermatitis and a high clinical suspicion of ACD, it may be beneficial to use the patients’ own products for patch testing in order to decrease the incidence of false-negative results.[17] In addition, strong consideration should also be given to testing with additional allergens, such as balsam of Tolu, fragrance mix 2, botanicals, and lichen acid mix, which may identify patients whose fragrance allergy would otherwise not be detected by standard fragrance allergens.
Propylene glycol, a solvent with moisturizing, antiseptic, and preservative properties, was the second most commonly present allergen and was present in 47 percent of the deodorants contained in the Walgreens database. It is used in a wide range of products, including cosmetics, food, toothpaste, and mouthwash, and functions in deodorants to stabilize the aqueous phase of the product. There is some controversy surrounding the allergic potential of PG. The NACDG found that 4.2 percent of patients referred for patch testing have a positive patch test to PG, but other studies have reported an incidence of positive reactions ranging from 0.1 to 3.8 percent.[18] This large variability may be due to the fact that PG is a strong irritant (the Material Safety Data Sheet advises avoidance at concentrations over 50 percent[11]); therefore, patch testing may yield false-positive reactions. This irritant property of PG is particularly relevant to antiperspirants and deodorants, where long-term occlusion in the underarm area may contribute to the induction of irritant dermatitis.10 Currently, the NACDG uses 30 percent PG in water for patch testing, a concentration that has significant potential for skin irritation.[19] At times, this irritation may be misinterpreted as contact dermatitis, leading to questionable data regarding true allergic potential of the product. To verify positive patch-test results, Funk et al suggest repeated patch test with serial dilutions, biopsies of affected skin, and oral challenge tests,[19] but these methods are rarely used in the clinical setting. Propylene glycol is commonly found in deodorants at a concentration of 2 to 5 percent of product weight.[20] This relatively low concentration may be below the elicitation threshold for some patients with PG allergy, but since it is difficult, if not impossible, to prospectively identify PG allergic patients who will tolerate PG-containing products and because their elicitation threshold may change over time, it is prudent to recommend that all patients with a positive patch test to PG avoid antiperspirants and deodorants containing this allergen.
Essential oils were present in 10 percent of the antiperspirants and deodorants analyzed in our search. Essential oils, naturally occurring mixtures of substances derived from plants, are frequently used fragrance ingredients. They have a highly variable composition of many different compounds and are known sensitizers. A recent study analyzed seven essential oils using the local lymph node assay for individual hazard assessment. This study looked at the seven essential oils used most commonly in fragrances and found basil oil to have the lowest concentration needed to elicit a positive response.[21] The same study also found that the three major components of essential oils—citral, eugenol, and geraniol—had similar elicitation potentials as their parent compound. Another found that ylang-ylang oil and lemongrass oil have significant abilities to induce sensitization.[22] These and other studies indicate that essential oils and their components are important allergens to consider when evaluating a patient with ACD.
Parabens were found in only two, or 1.8 percent, of deodorants analyzed in the Walgreens database. Parabens, including methyl paraben, ethyl paraben, butyl paraben, and propyl paraben, are preservatives used for their antibacterial and antifungal properties. They are generally efficacious, inexpensive, and safe. Although widely used, parabens can cause ACD in sensitized individuals. Paraben allergy is a relatively uncommon entity with rates of sensitization cited at 0 to 3.5 percent of the population. One study assessing cosmetic allergy in 1,937 patients found that only 0.3 percent reacted to patch testing with parabens.[23] In addition, the paraben paradox, a term coined by Fisher, implies that individuals who are allergic to parabens will often only have a reaction when the compound is applied to already inflamed skin and will not experience any reaction when it is applied to normal, nonirritated skin.[24,25] Parabens are frequently used in cosmetic products and perhaps the low frequency at which they were used in the deodorants we analyzed reflects a public perception that they may be related to the increasing incidence of breast cancer.[26] Although this concern may have lead manufacturers to avoid the use of parabens in antiperspirants and deodorants, it is important to note that this hypothesis linking parabens and breast cancer has not been proven and has been refuted by multiple studies.[27]
Vitamin E, or tocopherol, was found in two, or 1.8 percent, of the deodorants contained in our search. It is used as an inexpensive and natural preservative and at times is also added to beauty products due to the belief that it functions as an antioxidant and moisturizer. Vitamin E’s antioxidant properties have been attributed to its ability to remove free radicals and inhibit lipid peroxidation in cell membranes.[28] It has also been hypothesized to play a role in antiproliferative cell signaling events.[29] Although tocopherol is generally believed to be a benign addition to many beauty products, it can occasionally cause allergic dermatitis. In fact, the NACDG reported that 1.1 percent of those patch tested with dl-alpha-tocopherol experienced positive reactions, and there are several case reports of axillary dermatitis specifically related to tocopherol found in deodorant.[29,30] Although these infrequent cases illustrate the rarity of tocopherol-induced dermatitis, it is important to note that tocopherol may be responsible for more cases of ACD than recognized. For example, one large-scale outbreak of papular and follicular dermatitis occurred in Switzerland following the use of a new cosmetics line.[31] Perrenoud et al patch tested 77 of these patients and found that the agent responsible for the outbreak was tocopherol linoleate.[31] With this data in mind, they concluded that oxidized vitamin-E derivatives may be responsible for irritation to many cosmetic products.
Lanolin was present in one deodorant contained in the Walgreens database. Lanolin is a mixture of cholesterol and several fatty acid esters that are derived from the secretions of sheep sebaceous glands. Although the exact allergens are unknown, it has been proposed that wool alcohols are the main sensitizers present in lanolin.[32] Currently, 30-percent wool alcohol is recommended for patch testing patients with suspected lanolin allergy.[33] In the past, lanolin has been considered a significant source of allergy, and many products on the market are listed as lanolin-free. Recently these statistics have come into question. Wakelin et al proposed that the stated frequency of allergy is falsely elevated due to the fact that lanolin sensitivity was previously assessed in those individuals at high risk.[34] In a chart review of 24,449 patients patch tested with 30-percent wool alcohol, annual rates of sensitization of 1 to 7 percent were demonstrated, with an overall incidence of less than two percent in the patch-test population. Wakelin et al also commented on potential risk factors that might indicate future lanolin allergy, including female sex, increased age, lower leg venous stasis, and the presence of anogenital dermatitis. Several other studies have supported the suggestion that the true incidence of sensitivity to lanolin is quite low.[35–37] The NACDG reported an incidence of positive patch tests to lanolin of 2.2 percent in their 2001–2002 sample of patients. The rarity at which we found lanolin to be used in antiperspirants and deodorants, coupled with the rarity of sensitization to lanolin in the general population, suggests that ACD due to lanolin in deodorants is an infrequently encountered clinical problem.
Conclusion
Antiperspirants and deodorants are widely used cosmetic products and are frequently the cause of axillary dermatitis. Compounds contained in these products have the potential to cause irritant and allergic reactions in many consumers, making it important for doctors to be aware of the ingredients most likely to blame for these adverse reactions. Our search of the Walgreens database found that fragrance, PG, essential oils and biological additives, parabens, vitamin E, and lanolin were the most commonly used potential allergens in antiperspirants and deodorants. While it is important to keep these compounds in mind when assessing a patient with an underarm rash, it is often difficult to determine exactly which ingredient is to blame. Therefore, empirically recommending low allergenicity products, such as those contained in Table 2, may be beneficial for these patients. Also of note, new crystal products, which claim to be all natural and free of any additives, may also be useful in these patients. Unfortunately, axillary dermatitis is difficult to manage, and the problem may persist despite avoidance of common allergens. In these cases, further work-up with patch testing or biopsy may be warranted.
References
1. Benohanian A. Antiperspirants and deodorants. Clin Dermatol. 2001;19(4):398–405.
2. McGrath KG. An earlier age of breast cancer diagnosis related to more frequent use of antiperspirants/ deodorants and underarm shaving. Eur J Cancer Prev. 2003;12(6): 479–485.
3. Mirick DK, Davis S, Thomas DB. Antiperspirant use and the risk of breast cancer. J Natl Cancer Inst. 2002;94(20):1578–1580.
4. Ferreira PC, Piai Kde A, Takayanagui AM, Segura-Muñoz SI. Aluminum as a risk factor for Alzheimer’s disease. Rev Lat Am Enfermagem. 2008;16(1):151–157.
5. Graves AB, White E, Koepsell TD, et al. The association between aluminum-containing products and Alzheimer’s disease. J Clin Epidemiol. 1990;43(1): 35–44.
6. Montemarano AD, Sau P, Johnson FB, James WD. Cutaneous granulomas caused by an aluminum-zirconium complex: an ingredient of antiperspirants. J Am Acad Dermatol. 1997;37(3 Pt 1):496–498.
7. Orton DI, Wilkinson JD. Cosmetic allergy: incidence, diagnosis, and management. Am J Clin Dermatol. 2004;5(5):327–337.
8. Uter W, Geier J, Schnuch A, Frosch PJ. Patch test results with patients’ own perfumes, deodorants and shaving lotions: results of the IVDK 1998-2002. J Eur Acad Dermatol Venereol. 2007;21(3):374–379.
9. Watkinson A, Lee RS, Moore AE, et al. Is the axilla distinct skin phenotype? Int J Cosmet Sci. 2007;29(1):60.
10. Agren-Jonsson S, Magnusson B. Sensitization to propantheline bromide, trichlorocarbanilide and propylene glycol in an antiperspirant. Contact Dermatitis. 1976;2(2):79–80.
11. Scheman A, Jacob S, Zirwas M,et al. Contact allergy: alternatives for the 2007 North American contact dermatitis group (NACDG) Standard Screening Tray. Dis Mon. 2008;54(1-2):7–156.
12. Johansen JD. Fragrance contact allergy: a clinical review. Am J Clin Dermatol. 2003;4(11):789–798.
13. Johansen JD, Rastogi SC, Bruze M, et al. Deodorants: a clinical provocation study in fragrance-sensitive individuals. Contact Dermatitis. 1998;39(4):161–165.
14. Gerberick GF, Robinson MK, Felter SP, White IR, Basketter DA. Understanding fragrance allergy using an exposure-based risk assessment approach. Contact Dermatitis. 2001;45(6):333–340.
15. Lunder T, Kansky A. Increase in contact allergy to fragrances: patch-test results 1989-1998. Contact Dermatitis. 2000;43(2):107–109.
16. Kiec-Swierczynska M, Krecisz B, Swierczynska-Machura D. Allergy to cosmetics. I. Fragrances. Med Pr. 2004;55(2):203–206.
17. Daecke CM, Schaller J, Goos M. Value of the patient’s own test substances in epicutaneous testing. Hautarzt. 1994;45(5):292–298.
18. Lessmann H, Schnuch A, Geier J, Uter W. Skin-sensitizing and irritant properties of propylene glycol. Contact Dermatitis. 2005;53(5):247–259.
19. Funk JO, Maibach HI. Propylene glycol dermatitis: re-evaluation of an old problem. Contact Dermatitis. 1994;31(4):236–241.
20. World Intellectual Property Organization website. http://www.wipo.int/pctdb/en/ wo.jsp?IA=EP2005004828&wo=2005112879&DISPLAY=STATUS. Accessed August 30, 2008.
21. Lalko J, Api AM. Investigation of the dermal sensitization potential of various essential oils in the local lymph node assay. Food Chem Toxicol. 2006;44(5):739–746. Epub 2005 Dec 1.
22. Frosch PJ, Johansen JD, Menné T, et al. Further important sensitizers in patients sensitive to fragrances. Contact Dermatitis. 2002;47(5): 279–287.
23. Kiec-Swierczynska M, Krecisz B, Swierczynska-Machura D. Contact allergy to preservatives contained in cosmetics. Med Pr. 2006;57(3): 245–249.
24. Fisher AA. Esoteric contact dermatitis. Part I: the paraben paradox. Cutis. 1996;57(2):65–66.
25. Fisher AA. Esoteric contact dermatitis. Part II: the paraben paradox. Cutis. 1996;57(3):135–138.
26. Darbre PD, Aljarrah A, Miller WR, et al. Concentrations of parabens in human breast tumours. J Appl Toxicol. 2004;24(1):5–13.
27. Antiperspirant use and the risk of breast cancer. Journal of the National Cancer Institute. 2002;94(20): 1578–1580.
28. Packer L, Weber SU, Rimbach G. Molecular aspects of alpha-tocotrienol antioxidant action and cell signalling. J Nutr. 2001;131(2):369S–373S.
29. Minkin W, Cohen HJ, Frank SB. Contact dermatitis from deodorants. Arch Dermatol. 1973;107(5):774–775.
30. Aeling JL, Panagotacos PJ, Andreozzi RJ. Allergic contact dermatitis to vitamin E aerosol deodorant [letter]. Arch Dermatol. 1973;108(4):579–580.
31. Perrenoud D, Homberger HP, Auderset PC, et al. An epidemic outbreak of papular and follicular contact dermatitis to tocopheryl linoleate in cosmetics. Swiss Contact Dermatitis Research Group. Dermatology. 1994;189(3): 225–33.
32. Oleffe JD, Blondeel A, Broschmans L. Patch testing with lanolin. Contact Dermatitis. 1978;4:233.
33. Hjorth N, Trolle-Larsen C. Transactions of the St. John’s Hospital Dermatological Society. 1963;49:127.
34. Wakelin SH, Smith H, White IR, Rycroft RJ, McFadden JP. A retrospective analysis of contact allergy to lanolin. Br J Dermatol. 2001;145(1):28–31.
35. Epstein E. The detection of lanolin allergy. Arch Dermatol. 1972;106:678–681.
36. Holness DL, Nethercott JR, Adams RM, et al. Concomitant positive patch test results with standard screening tray in North America 1985–1989. Contact Dermatitis. 1995;32:289–292.
37. Christophersen J, Menne T, Tanghoj P, et al. Clinical patch test results analyzed by multivariate analysis. Contact Dermatitis. 1989;21:291–299.