
James Q. Del Rosso, DO, FAOCD
Clinical Professor (Dermatology), Adjunct Faculty, Touro University College of Osteopathic Medicine, Henderson, Nevada and Private Practice, Dermatology and Cutaneous Surgery/Mohs Micrographic Surgery and Las Vegas Skin & Cancer Clinic/West Dermatology Group,
Henderson and Las Vegas, Nevada
Abstract
Onychomycosis is a common infection of the nail unit that is usually caused by a dermatophyte (tinea unguium) and most frequently affects toenails in adults. In most cases, onychomycosis is associated with limited treatment options that are effective in achieving complete clearance in many cases. In addition, recurrence rates are high in the subset of treated patients who have been effectively cleared, usually with an oral antifungal agent. There has been a conspicuous absence of medical therapies approved in the United States since the introduction of topical ciclopirox (8% nail lacquer), with no new effective agents introduced for more than 10 years. Fortunately, newer agents and formulations have been under formal development. While patients might prefer a topical therapy, efficacy with ciclopirox 8% nail lacquer, the only available agent until the very recent approval of efinaconazole 10% solution, has been disappointing. The poor therapeutic outcomes achieved with ciclopirox 8% nail lacquer were not unexpected as the cure rates achieved in the clinical trials were unimpressive, despite concomitant nail debridement, which was an integral part of the pivotal trials with ciclopirox 8% nail lacquer. Efinaconazole 10% solution and tavaborole 5% solution are new topical antifungals specifically developed for the treatment of dermatophyte onychomycosis. In Phase 3 clinical trials, both newer agents were applied once daily for 48 weeks without concomitant nail debridement. Mycologic cure rates with efinaconazole 10% solution are markedly superior to what was achieved with ciclopirox 8% nail lacquer. To add, they appear to be nearly comparable to those achieved with oral itraconazole in pivotal clinical trials. However, it is important to remember that direct comparisons between different studies are not conclusive, are not generally considered to be scientifically sound, and may not be entirely accurate due to differences in study design and other factors. Well-designed and properly powered head-to-head studies are needed in order to draw definitive conclusions about efficacy comparisons between therapies, at least based on academic and regulatory standards. Although tavaborole 5% solution is in an earlier phase of development for onychomycosis, treatment success rates reported thus far for both efinaconazole 10% solution and tavaborole 5% solution are superior to ciclopirox 8% nail lacquer. As a result, a new era of onychomycosis appears to be upon us that incorporates topical therapy more effectively than in the past. Not only may these newer topical agents provide viable monotherapy alternatives to oral therapy for onychomycosis, topical therapy for onychomycosis that is effective, well tolerated, and easy to use may also find a role in combination therapy, and/or as continued therapy after initial clearance to reduce recurrence or re-infection. (J Clin Aesthet Dermatol. 2014;7(7):10–18.)
Onychomycosis is the most common fungal infection of the nail bed, matrix, and/or plate, representing up to 50 percent of all nail disorders seen in dermatology practice.[1] Overall prevalence, noted to be approximately 14 percent, appears to be increasing, with onychomycosis reported to affect half the population by the time they reach 70 years of age.[2–5] Left untreated, it can lead to progressive destruction and deformity of the toenails and fingernails.[1,6] Onychomycosis, especially cases caused by dermatophytes, may serve as a nidus for more widespread cutaneous involvement, spreading to other digits, body areas, and even to other predisposed family members.[7] It can be very distressing for many patients psychosocially and/or physically.[5,8–10]
Causes of onychomycosis. The vast majority of cases of onychomycosis are caused by dermatophyte fungi. In 80 to 98 percent of affected individuals, Trichophyton rubrum or Trichophyton mentagrophytes are identified as the causative pathogen.[11–14] Adults are most commonly affected with toenails being affected much more commonly than fingernails.[1,3–5,11–14] Fingernail onychomycosis is frequently concomitant with toenail onychomycosis, especially when a dermatophyte is causative, and most of these patients exhibit concurrent unilateral or bilateral dry plantar (moccasin) tinea pedis and sometimes also tinea manus. Both fingernail and toenail onychomycosis can occasionally be caused by nondermatophyte fungi, such as Scopulariopsis brevicaulis, Aspergillus spp, Fusarium spp, and sometimes Candida spp (i.e., C. albicans), with the latter noted to be rare in toenails.[15] Increasing prevalence of nondermatophyte onychomycosis has been observed in some reports, either due to improved diagnostic techniques and/or increased awareness; however, differentiation of a laboratory contaminant from a true nail pathogen may at times be overlooked and/or problematic.[16,17] In addition, mixed infections have been reported, although their significance is less clear.[18] Identification of the fungal pathogen by culture is highly dependent on the method used to obtain the specimen, the anatomic location within the nail unit that the specimen is obtained from, and the medium used.
Patterns of nail invasion/clinical presentations of onychomycosis. Toenail onychomycosis frequently involves several nails, and as noted above, dry plantar tinea pedis is almost always present concurrently.[11,19,20] Indeed, tinea pedis is believed to be the predominant source of dermatophyte onychomycosis. This occurs in most cases as Trichophyton spp (usually T. rubrum) migrates from distal pedal skin into nail bed by violating the hyponychium. As a result, distal lateral subungual onychomycosis (DLSO) is by far the most common form of the disease.[1,3,5,11–14] Here the causative fungus, usually T. rubrum, invades the nail bed at the distal and lateral edges, leading to distal onycholysis, subungual hyperkeratosis, and both nail bed and nail plate thickening.[21] This subungual process of nail invasion by the fungal pathogen is the most common, with direct nail plate (endonychial) invasion much less common, especially with dermatophyte fungi.[3,5,11,15] In DLSO, the undersurface of the nail plate is often affected by fungal penetration as it is directly contiguous with the invaded nail bed. Onychomycosis involving the surface of the nail plate (superficial onychomycosis) is also usually caused by Trichophyton spp, is much less common, and sits on the surface of the plate as a powdery film that can be scraped away from that surface with a surgical blade or lightly with a curet. Superficial dermatophyte onychomycosis is amenable to topical therapy as the fungal pathogen is easily accessible to the applied antifungal agent.[3,5,11,15] Proximal subungual onychomycosis is also less common than DLSO and occurs when the dermatophyte organism (usually Trichophyton spp) migrates from pedal skin under the proximal nail fold and cuticle and extends under the nail plate and into the nail bed.[3,5,11,15]
Challenges in treating onychomycosis. Successful treatment of onychomycosis is fraught with difficulty due to several factors, especially with toenail involvement. These include slow growth; the physical presence of the nail plate interfering with nail bed access after application of a topical antifungal agent; difficulty in finding compounds with the pharmacologic/pharmacokinetic profile to allow adequate nail unit penetration; challenges in achieving therapeutic substantivity of drug levels after topical or oral administration; development of optimal vehicles for topical use that allow delivery of effective drug levels to the site(s) of nail infection (primarily nail bed); the anatomic nature of the nail unit and its vascular access, which allows for higher drug levels in nail bed/plate centrally as compared to laterally after oral antifungal administration; the high incidence of recurrence after clearance with therapy; widespread environmental exposure to dermatophytes and other fungal organisms; and the genetic predisposition of many individuals to pedal colonization and infection with T. rubrum, which eventually leads to invasion of the nail unit with reinfection with onychomycosis (tinea unguium).[1,3,5,7,12,16,19,21–23] Toenails may take up to 78 weeks to grow out completely, depending on the age and general health of the patient.[22,23] In addition, certain clinical presentations of onychomycosis are more difficult to clear and often represent cases that are not included in many clinical studies, including some pivotal trials. These include marked nail plate thickening, extensive onycholysis, completely affected nail plate with marked involvement of the nail matrix, dermatophytomas, band-like lateral involvement, extensive subungual debris/thickening, lack of nail growth of chronically traumatized toenails (i.e., 5th, 2nd if longest toe), and immunocompromised patients. Such cases often involve physical debridement combined with medical therapy, and may warrant repeated courses of treatment and/or more prolonged therapy than what is stated in product labeling.[1,3,5,24–28]
Poor nail unit penetration limits the use of current topical antifungal agents in the treatment of onychomycosis and directly relates to the unique physical and kinetic properties of the nail unit, its thickness, and relatively compact structure.[24–26] Due to the high potential for persistence of some organisms within the nail unit even after visible clearance and/or dermatophyte presence on pedal skin, relapse and re-infection of onychomycosis are common and can occur in at least 20 to 25 percent of patients.[1,3,5,19,20,22,23,27]
Oral treatment considerations. Current treatment of dermatophyte onychomycosis includes both oral and topical antifungal agents, adjunctive physical modalities (chemical debridement, mechanical debridement, nail avulsion), and approaches to minimize the risk of recurrence or re-infection (i.e., topical therapy to suppress pedal colonization or infection [tinea pedis]).[28] Oral antifungal therapy, such as with agents approved by the United States (US) Food and Drug Administration (FDA) for dermatophyte onychomycosis (i.e., terbinafine, itraconazole), is preferred because of their ability to penetrate the nail bed and nail plate and sustain therapeutic levels that correlate with markedly superior efficacy as compared to oral griseofulvin. This latter oral agent was the first to become FDA-approved for dermatophyte infections, including onychomycosis, despite a very low cure rate for tinea unguium even with several months of daily therapy (especially toenails).[1,3,5] Nevertheless, oral antifungal monotherapy for toenail dermatophyte onychomycosis is still not capable of clearing many cases due to the reasons explained above. In addition, there are safety concerns (i.e., hepatotoxicity) that warrant monitoring and a risk of clinically significant drug interactions, especially with itraconazole. These factors can be of greater concern in elderly patients with onychomycosis where polypharmacy is common. In many cases, both patient and physician preference for an effective topical solution exists. In some cases, the clinician may wish to combine oral and topical therapy.
Approved topical agents for onychomycosis. There have been a number of failed topical therapies in development over the last 10 to 15 years. Until June 6, 2014, only one topical agent, ciclopirox 8% nail lacquer, was FDA approved and available in the United States for treatment of onychomycosis. Efficacy has been disappointing, resulting in topical ciclopirox usually being used for the mildest cases; only for palliative benefit at best; or when oral therapy cannot be tolerated, is best avoided, or is contraindicated.[29] This review highlights the data with “standard” regimens of oral therapy and provides an overall comparison of their efficacy and safety profiles with existing and newer topical agents in development. There are a number of important aspects to consider in reviewing efficacy data from onychomycosis studies. First, mycologic cure (i.e., the eradication of the causative organism) is the only consistently defined efficacy parameter applied to toenail onychomycosis clinical trials that is objective,[22] and it is widely accepted that mycologic cure is the main treatment goal.[30] Clinical cure (completely normal-appearing nail at study endpoint) is also a very important goal, but is fraught with the complication of pre-existing nail changes unrelated to onychomycosis (i.e., trauma-related). Secondly, the duration of treatment in clinical trials can suggest lower efficacy rates than would be the case with continued treatment when elected by a clinician in “real-world” clinical practice. In many cases of toenail onychomycosis, prolonged or repeated therapy is needed to achieve resolution of the disease, given the slow growth of the toenail mentioned earlier, and also the propensity for continued re-exposure to the fungal pathogen over time, especially in those with pedal colonization by T. rubrum. Continued improvement has been reported with longer-term studies, although data are somewhat limited.[31] Thirdly, the use of an adjunctive physical modality such as debridement may be needed in combination with medical therapy to augment the therapeutic response based on the clinical presentation of onychomycosis. Finally, while most studies have defined disease severity based on the percent involvement of the affected target toenail, there is no consistency in defining severity of a condition where a number of other factors (i.e., proximity of infection to the matrix, degree of subungual hyperkeratosis, presence of dermatophytoma, extent of onycholysis, multiple nail involvement, associated tinea pedis) are important in assessing severity and selecting therapy.[32]
Oral Antifungal Therapy For Toenail Onychomycosis
It is not suggested that oral griseofulvin be used for dermatophyte onychomycosis in adults due to poor efficacy, and oral ketoconazole is also not suggested for onychomycosis treatment due to poor efficacy and safety concerns. Oral terbinafine (250mg daily for 12 weeks) and itraconazole “pulse” therapy (200mg given twice daily for 1 week per month) have been shown to be the most effective dermatophyte onychomycosis regimens, although the latter regimen is not FDA-approved for toenail onychomycosis. Itraconazole (FDA approval 1995) and terbinafine (FDA approval 1996) offer mycologic cure rates of 54 and 70 percent, respectively, following continuous therapy as reported in their approved product labeling.[33,34].
Few comparative studies have evaluated the relative efficacy of these two regimens[35–38]; however, the literature suggests superiority of terbinafine or comparable efficacy.[28] Studies suggest that at least 20 to 30 percent of patients with toenail dermatophyte onychomycosis may not respond adequately to initial therapy with terbinafine or pulsed itraconazole.[39] A comprehensive meta-analysis compared the efficacy of continuous and pulsed itraconazole with terbinafine and reported mycologic cure rates of 71.1±5.0, 65.5±5.1, and 77.2±4.0 percent, respectively.[39] A more recent cumulative meta-analysis of randomized clinical trials from the same group reported mycologic cure rates of 63±7 percent with itraconazole pulse, 76±3 percent with terbinafine, and 48±5 percent with fluconazole.[40] Fluconazole has been shown to be effective for dermatophyte onychomycosis, but is not FDA-approved for any type of onychomycosis.
Standard courses of itraconazole and terbinafine have been shown to achieve a disease-free nail in approximately 25 to 40 percent and 35 to 50 percent of patients, respectively.[41] Nail infections are difficult to cure, with rates of recurrence of 33.7 and 11.9 percent being reported for itraconazole and terbinafine, respectively, after long-term follow-up.[42] After five years, 46 percent of patients treated with terbinafine remained disease-free compared with just 13 percent of patients treated with itraconazole.[43]
Although most studies with oral terbinafine and itraconazole have been for treatment of dermatophyte infections, efficacy against nondermatophyte infections, reported to affect 1.5 to 22 percent of patients, is an important consideration when selecting treatment for onychomycosis.[44,45] In many cases, itraconazole appears to be more effective overall for nondermatophyte nail pathogens.[45,46] Treatment of C. albicans onychomycosis, which almost always involves fingernails as opposed to toenails, suffers lower efficacy when treated with oral terbinafine.[46,47]
Topical Antifungal Therapy For Toenail Dermatophyte Onychomycosis
Prior to the development of topical efinaconazole and tavaborole for onychomycosis, available topical agents have exhibited limited nail unit penetration and very poor efficacy. Cure rates, alone or in combination with physical modalities, such as debridement or avulsion, have been modest at best.[28] The daily application of ciclopirox 8% nail lacquer used in combination with nail plate debridement may be effective in some patients with milder severity of disease if treatment continues until the nail plate grows out completely.[48] However, ciclopirox 8% nail lacquer with nail debridement has only rarely been effective with a reported mycologic cure rate (negative culture and negative potassium hydroxide preparation [KOH]) range of 29 to 36 percent.[49,50] This mycologic cure rate range is out of step with complete cure rates (mycologic cure and normal-appearing toenail) reported to range from 5.5 to 8.5 percent.[50] There is a definite need for an effective and safe topical product that can adequately penetrate the toenail plate and nail bed and inhibit the growth of fungi that cause onychomycosis.
New Topical Solutions for the Treatment of Toenail Onychomycosis
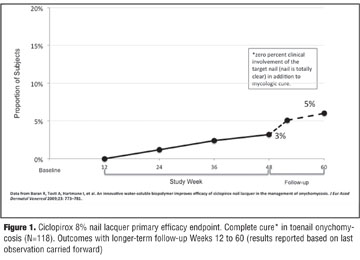
There have been a number of failed development programs over the last 10 to 15 years as researchers attempt to formulate antifungals that show in vitro activity against the common pathogens that cause onychomycosis and to penetrate the nail unit with adequate access to the site of infection. The logical place to start is with the oral antifungal agents already being used to effectively treat dermatophyte onychomycosis. A topical formulation of terbinafine demonstrated mycological and clinical efficacy in vitro and was superior to topical ciclopirox in a Phase 2 study.[51,52] However, Phase 3 studies failed to demonstrate superior efficacy in mild-to-moderate DLSO compared to vehicle in terms of complete cure.[53] In two vehicle-controlled studies, mycologic cure rates with terbinafine were 13 and 19 percent (P=0.014 and P<0.0001, respectively, compared to vehicle) after 24 and 48 weeks of treatment. Complete cure rates were only 1.2 and 2.2 percent after 24 and 48 weeks of treatment with terbinafine solution and not significantly different than vehicle. The third study was an active-comparator controlled study with amorolfine 5% nail lacquer with both treatments administered over 48 weeks. Mycologic cure rates were 16 percent in both study groups and complete cure rates were very low in both the terbinafine study arm and amorolfine study arm (1.2 and 0.96%, respectively).[53] Although the results reported for amorolfine are lower than those reported in earlier studies, there are important methodological differences, including less strictly defined endpoints and lack of control groups in previous studies.[54,55] One concern expressed by some investigators is the short duration of studies using topical treatments given the slow growth rate of toenails, suggesting that a treatment duration of 18 months is required to achieve both clinically meaningful and demonstrable benefit.[53] Studies with oral antifungal agents have demonstrated higher cure rates and greater clinical benefit following long-term (72 weeks) treatment.[31] Improvement in cure rates with longer follow-up periods as compared to the usually reported durations (i.e., 4 weeks) has been observed with topical therapy. In one multicenter study, the complete cure at Week 52 following 48 weeks of therapy with ciclopirox 8% nail lacquer in mild-to-moderate DLSO was 3.2 percent and at Week 60 had increased to 5.8 percent (Figure 1).[56] Interestingly in this study, which stated a primary objective to see if formulation improvements can enhance efficacy rates, the secondary endpoint of “responder rate,” defined as a decrease in diseased nail to ?10 percent of total, did not increase over a more prolonged follow-up period. The “responder rate” was 17.3 percent at both follow up points.[56]
The development of new topical antifungal agents for the treatment of onychomycosis has focused on formulation enhancements and also the discovery of new chemical entities that exhibit a broad spectrum of activity against multiple relevant fungal pathogens and that exhibit the pharmacological characteristics that are needed for effective treatment of toenail onychomycosis. This review focuses primarily on efinaconazole 10% topical solution, which has been evaluated in mandatory studies and clinical trials required for submission to the FDA, and was recently FDA approved in June 2014 for toenail dermatophyte onychomycosis.[57] Topical tavaborole is also under evaluation by the FDA for treatment of toenail onychomycosis although data from clinical trials was not available at the time this article was written and accepted for publication.
Efinaconazole. Efinaconazole 10% solution has shown efficacy based on mycologic and complete cure that appear based on an overall assessment to be relatively comparable to rates reported with oral itraconazole in some studies for mild-to-moderate DLSO and greater than those reported with ciclopirox 8% nail lacquer combined with debridement.[29,57] Physicochemical properties, antifungal activity, and the nature of the vehicle formulation are components that are believed to contribute to favorable therapeutic outcomes in onychomycosis patients.[58,59]
Efinaconazole has a broad spectrum of in vitro activity against dermatophytes, nondermatophytes, and yeasts. Against the most common pathogens, T. rubrum and T. mentagrophytes (MIC90: 0.008–0.015 µg/mL) and C. albicans (MIC50: 0.004 µg/mL), it was more potent than currently marketed antifungal agents used to treat onychomycosis.[60] Efinaconazole 10% solution was also significantly superior to amorolfine (P<0.001) and ciclopirox (P<0.01) lacquers in decreasing the number of dermatophytes in an in vivo guinea pig model of onychomycosis.[59]
The physicochemical properties of a topical antifungal need to be favorable for its penetration through the dense keratinized nail plate to its deeper layers, into nail bed and into nail matrix. Many antifungal agents are known to possess a high binding affinity to keratin that can have a counteractive effect on their efficacy by reducing the availability of free drug.[61–63] Both keratin binding and the rate of drug release from keratin are important considerations in allowing the antifungal agent to become freely accessible to exert its activity against causative fungal organisms.
Efinaconazole 10% solution has considerably lower binding to keratin, and keratin-bound drug was released at a faster rate following repeated washings (85.7% bound; 46% released) when compared to amorolfine (98.1% bound, 6.9% released) and ciclopirox (99.3% bound, 2.4% released).[59] Efinaconazole 10% solution is a clear solution containing alcohol, lipophilic esters, and cyclomethicone. These ingredients help to create a low surface tension ideal for application to the dry nail plate surface, lateral and proximal nail folds, hyponychium, and the undersurface of the nail plate that is accessible due to distal onycholysis.[58] The efinaconazole concentration is maintained in a dissolved state after the evaporation of the volatile vehicle components. Unlike previous lacquer-based treatments, such as ciclopirox 8%, reported efficacy data with efinaconazole 10% solution reflect use without concomitant nail debridement between applications.
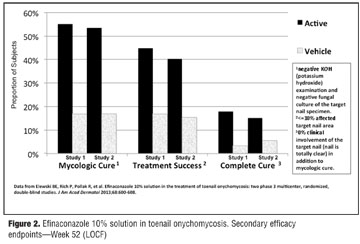
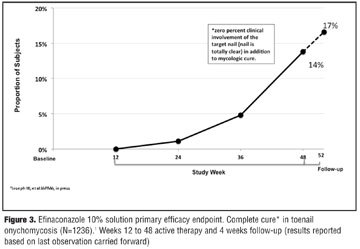
Efficacy of efinaconazole 10% solution was evaluated in two Phase 3 studies of 1,655 subjects with mild-to-moderate DLSO over 48 weeks, with a four-week follow-up. At Week 52, 55.2% (study 1) and 53.4% (study 2) of subjects achieved mycologic cure with efinaconazole 10% solution compared to 16.8 and 16.9 percent with vehicle, respectively (Figure 2).57 At Week 52, 40 to 45 percent of subjects were considered treatment successes, defined as affected target toenail area of ?10 percent, with efinaconazole 10% solution compared to vehicle (Figure 2, P<0.001). Complete cure rates with efinaconazole 10% solution were almost 17 percent (Figure 3).[57]
Tavaborole. Tavaborole represents a new class of protein synthesis inhibitors that exhibit antifungal properties.[64] Two Phase 3 studies in patients with mild-to-moderate DLSO treated with topical tavaborole have recently been completed, although the data was not available at the time this article was written and accepted for publication. As with efinaconazole 10% solution, topical tavaborole is reported to be markedly superior to ciclopirox 8% nail lacquer for dermatophyte onychomycosis. Evaluation of the study details with topical tavaborole await the publication of outcomes from clinical studies.
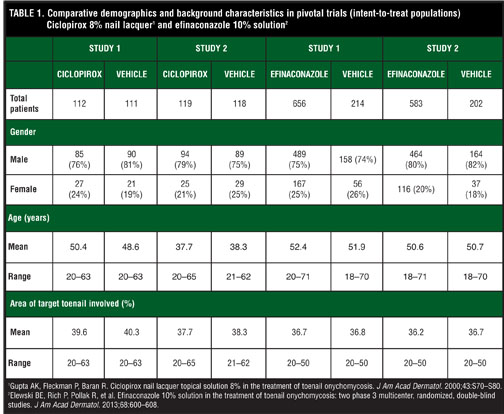
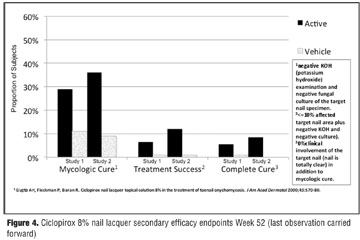
Comparisons of efinaconazole and ciclopirox. It is not entirely accurate to directly compare the efficacy of efinaconazole 10% solution with ciclopirox 8% nail lacquer for dermatophyte toenail onychomycosis. However, the baseline demographics and overall inclusion characteristics in the pivotal studies with these two compounds were very similar (Table 1), thus allowing for some overall general comparisons and qualitative differences between these two agents.[48,50,57] A major difference of note between trials with both agents was the younger patient population in the second ciclopirox study, which may be one reason behind the better results seen in this study as compared to the first study with ciclopirox. Mycologic cure, complete cure, and treatment success with ciclopirox 8% nail lacquer are summarized in Figure 4. Mycologic cure rates with ciplopirox 8% nail lacquer (29–36%) are lower than those reported with efinaconazole 10% solution (53–55%) and complete cure rates (5.5–8.5% versus 15.8–17.2%) are twofold to threefold lower, despite concomitant nail debridement with ciclopirox and not with efinaconazole. Given the slow toenail growth, treatment success (defined as ?10% clinical involvement) may be a realistic and helpful gauge of the therapeutic value of topical agents in clinical practice, especially if one considers using a longer course of therapy than 48 weeks. Treatment success based on the aforementioned definition was achieved in 40 to 45 percent of subjects treated with efinaconazole 10% solution. The mean percent toenail involvement at baseline in the efinaconazole studies was 36 percent, with almost half of the patients showing ?10 percent toenail involvement at the end of the study.[57] With ciclopirox 8% nail lacquer, 7 to 12 percent of subjects achieved treatment success; however, the definition of “treatment success” in the ciclopirox studies included mycologic cure, thus making even a general comparison difficult (Figures 2 and 3).65 Overall, efinaconazole 10% solution and ciclopirox 8% nail lacquer were safe and well-tolerated.[48,50,57,65]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Conclusion
Onychomycosis is a common nail disease that is challenging to treat successfully, and therapeutic choices are limited. Oral therapy has been the standard of care for the majority of our patients primarily because of the poor efficacy seen with previously used topical treatment. The availability of an effective, well-tolerated, topical antifungal would be particularly helpful, but options have not been forthcoming because of formulation difficulties hampering effective nail penetration to the site of infection. The development of new topical antifungals for onychomycosis has focused on the following three areas: topical formulations of current oral agents, new formulations of existing topical agents, and new chemical entities. Both the physicochemical properties of the agent and its formulation contribute to efficacy. Two new topical antifungals, efinaconazole 10% solution and tavaborole 5% solution, both appear to offer advantages over ciclopirox 8% nail lacquer, although it is not possible to directly compare the three topical products definitively. Efinaconazole 10% solution applied once daily without nail debridement provides mycologic and complete cure rates 2 to 3 times greater than those reported with ciclopirox 8% nail lacquer applied once daily with nail debridement in a very similar patient population. Based on data available to date, efinaconazole 10% topical solution appears to represent an important advance in the initial treatment and long-term management of this common toenail infection that is often progressive and debilitating.
Disclosure
Dr. Del Rosso serves as a consultant (C) and/or speaker (S) for several companies that currently market and/or are developing antifungal products, products used for management of onychomycosis, and/or other nail disorders, including Valeant [C,S] (efinaconazole 10% topical solution), Anacor [C,S] (tavaborole 5% solution), Innocutis [C,S], Merz [C,S], Quinnova [C], and Ranbaxy [C,S].
Acknowledgment
Brian Bulley, MSc (Inergy Limited, UK), provided assistance with the development of this manuscript. Medicis, a division of Valeant Pharmaceuticals, provided funding for the support provided by Inergy Limited, UK.
References
1. Scher RK, Coppa LM. Advances in the diagnosis and treatment of onychomycosis. Hosp Med. 1998;34:11–20.
2. Ghannoum MA, Hajjeh RA, Scher R,et al. A large-scale North American study of fungal isolates from nails: the frequency of onychomycosis, fungal distribution, and antifungal susceptibility patterns. J Am Acad Dermatol. 2000;43(4):641–648.
3. Elewski BE. Onychomycosis: pathogenesis, diagnosis, and management. Clin Microbiol Rev. 1998;11:415–429.
4. Elewski BE, Charif MA. Prevalence of onychomycosis in patients attending a dermatology clinic in northeastern Ohio for other conditions. Arch Dermatol. 1997;133:1172–1173.
5. Scher RK. Onychomycosis: therapeutic update. J Am Acad Dermatol. 1999;40:S21–S26.
6. Crissey JT. Common dermatophyte infections. A simple diagnostic test and current management. Postgrad Med. 1998;103(2):191–1,197–200,205.
7. Seebacher C, Brasch J, Abeck D, et al. Onychomycosis. Mycoses. 2007;50:321–327.
8. Drake LA, Patrick DL, Fleckman P, et al. The impact of onychomycosis on quality of life: development of an international onychomycosis questionnaire to measure patient quality of life. J Am Acad Dermatol. 1999;41:189–196.
9. Lubeck DP, Patrick DL, McNulty P, et al. Quality of life of persons with onychomycosis. Qual Life Res. 1993;2:341–348.
10. Whittam LR, Hay RJ. The impact of onychomycosis on quality of life. Clin Exp Dermatol. 1997;22:87–89.
11. Gupta AK, Jain HC, Lynde CW, et al. Prevalence and epidemiology of onychomycosis in patients visiting physicians’ offices: a multicenter Canadian survey of 15,000 patients. J Am Acad Dermatol. 2000;43:244–248.
12. Loo DS. Onychomycosis in the elderly: drug treatment options. Drugs Aging. 2007;24:293–302.
13. Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol. 2004;50:748–752.
14. Vender RB, Lynde CW, Poulin Y. Prevalence and epidemiology of onychomycosis. J Cutan Med Surg. 2006;10(Suppl 2):S28–S33.
15. Gupta AK, Ricci M-J. Diagnosing onychomycosis. Dermatol Clin. 2006;24:365–369.
16. Gupta AK, Ryder JE, Baran R, et al. Non-dermatophyte onychomycosis. Dermatol Clin. 2003;21(2):257–268.
17. Gupta AK, Drummond-Main C, Cooper EA, et al. Systematic review of nondermatophyte mold onychomycosis: diagnosis, clinical types, epidemiology, and treatment. J Am Acad Dermatol. 2012;66:494–502.
18. Summerbell RC. Epidemiology and ecology of onychomycosis. Dermatology. 1997;194(Suppl 1):32–36.
19. Roberts DT. Onychomycosis: current treatment and future challenges. Br J Dermatol. 1999;141(Suppl 56):1–4.
20. Lauritz B. Dermatoses of the feet. Am J Clin Dermatol. 2000;1:181–186.
21. Hay RJ, Baran R. Onychomycosis: a proposed revision of the clinical classification. J Am Acad Dermatol. 2011;65:1219–1227.
22. Werschler WP, Bondar G, Armstrong D. Assessing treatment outcomes in toenail onychomycosis clinical trials. Am J Clin Dermatol. 2004;5:145–152.
23. De Cuyper C. Long-term outcomes in the treatment of toenail onychomycosis. Br J Dermatol. 1999;141:15–20.
24. Baran R, Kaoukhov A. Topical antifungal drugs for the treatment of onychomycosis: an overview of current strategies for monotherapy and combination therapy. J Eur Acad Dermatol Venereol. 2005;19(1):21–29.
25. Lecha M, Effendy I, Feuilhade de Chauvin M, et al. Treatment options—development of consensus guidelines. J Eur Acad Dermatol Venereol. 2005;19(Suppl 1):25–33.
26. Murdan S. Drug delivery to the nail following topical application. Int J Pharm. 2002;236:1–26.
27. Gupta AK, Simpson FC. New therapeutic options for onychomycosis. Expert Opin Pharmacother. 2012;13(8): 1131–1142.
28. Del Rosso JQ. Current management of onychomycosis and dermatomycosis. Curr Infect Dis Rep. 2000;2(5):438–445.
29. Gupta AK, Joseph WS. Ciclopirox 8% nail lacquer in the treatment of onychomycosis of the toenails in the United States. J Am Podiatr Med Assoc. 2000;90:495–501.
30. Gupta AK. Treatment of dermatophyte toenail onychomycosis in the United States: a pharmacoeconomic analysis. J Am Podiatr Med Assoc. 2002;92:272–286.
31. Sigurgeirsson B, Billstein S, Rantanen T, et al. LION Study: efficacy and tolerability of continuous terbinafine (Lamisil) compared to intermittent itraconazole in the treatment of toenail onychomycosis: Lamisil vs. itraconazole in onychomycosis. Br J Dermatol. 1999;141(Suppl):5–14.
32. Carney C, Tosti A, Daniel R, et al. A new classification system for grading the severity of onychomycosis: Onychomycosis Severity Index. Arch Dermatol. 2011;147(11):1277–1282.
33. Sporanox (itraconazole) [package insert]. Titusville, NJ: Janssen; 2012.
34. Lamisil (terbinafine HCl) [package insert]. East Hanover, NJ: Novartis; 2012.
35. Kedja J. Itraconazole pulse therapy vs continuous terbinafine dosing for toenail onychomycosis. Postgrad Med. 1999;106(Suppl):12–15.
36. Bahadir S, Insioz HS, Cilsal G, et al. Continuous terbinafine or pulse itraconazole: a comparative study on onychomycosis. J Dermatol Treat. 1998,9:271.
37. Evans EG, Sigurgeirsson B: Double blind, randomized study of continuous terbinafine compared with intermittent itraconazole in treatment of toenail onychomycosis: the LION study group. BMJ. 1999;318:1031–1035.
38. Negroni R, Arechvala A, Bonvehi P, et al. Treatment of onychomycosis due to mycelial fungi. Revista Argentina de Micologia. 1998;21:8–14.
39. Gupta AK, Lambert J: Pharmacoeconomic analysis of the new oral antifungal agents used to treat toenail onychomycosis in the USA. Int J Dermatol. 1999;39(Suppl 2):53–64.
40. Gupta AK, Ryder JE, Johnson, AM. Cumulative meta-analysis of systemic antifungal agents for the treatment of onychomycosis. Br J Dermatol. 2004;150:537–544.
41. Epstein E. How often does oral treatment of toenail onychomycosis produce a disease-free nail. Arch Dermatol. 1998;134:1551–1554.
42. Piraccini BM, Sisti A, Tosti A. Long-term follow-up of toenail onychomycosis caused by dermatophytes after successful treatment with systemic antifungal agents. J Am Acad Dermatol. 2010;62:411–414.
43. Sigurgeirsson B, Olafsson JH, Steinsson JB, et al. Long-term effectiveness of treatment with terbinafine versus itraconazole in onychomycosis. Arch Dermatol. 2002;138:353–357.
44. Jain S, Sehgal VN. Onychomycosis: an epidemio-etiologic perspective. Int J Dermatol. 2000;39:100–103.
45. Greer DL. Evolving role of non-dermatophytes in onychomycosis. Int J Dermatol. 1995;34:521–529.
46. Del Rosso JQ, Gupta AK. The use of intermittent itraconazole therapy for superficial mycotic infections: a review and update on the “one week” approach. Int J Dermatol. 1999;38(Supp 2):28–39.
47. McClellan KJ, Wiseman LR, Markham A. Terbinafine: an update of its use in superficial mycoses. Drugs. 1999;58:179–202.
48. Bonifaz A, Barba Gomez F, Rodriguez G, et al: Multicenter study of the efficacy and security of ciclopirox lacquer 8% in onychomycosis. Dermatol Rev Mex. 1998;42:95–101.
49. de Berker D. Fungal nail disease. N Engl J Med. 2009;360:2108–2116.
50. Gupta AK, Joseph WS. Ciclopirox 8% nail lacquer in the treatment of onychomycosis of the toenails in the United States. J Am Podiatr Med Assoc. 2000;90:495–501.
51. Ghannoum MA, Long L, Pfister WR. Determination of the efficacy of terbinafine hydrochloride nail solution in the topical treatment of dermatophytosis in a guinea pig model. Mycoses. 2009;52:35–43.
52. Gupta A, Robbins J, Pfister W. Terbinafine nail solution is highly effective for the treatment of onychomycosis: a double-blind, randomized, dose-finding clinical trial. Paper presented at: Annual Scientific Meeting of Am Podiatr Med Assoc 2008; July 24–27; Honolulu, Hawaii.
53. Elewski BE, Ghannou MA, Mayser P, et al. Efficacy, safety and tolerability of topical terbinafine nail solution in patients with mild-to-moderate toenail onychomycosis: results from three randomized studies using double-blind vehicle-controlled and open-label active-controlled designs. J Eur Acad Dermatol Venereol. 2011 December 20. [Epub ahead of print].
54. Reinel D. Topical treatment of onychomycosis with amorolfine 5% nail lacquer: comparative efficacy and tolerability of once and twice weekly use. Dermatology. 1992;184(Suppl 1):21–24.
55. Lauharanta J. Comparative efficacy and safety of amorolfine nail lacquer 2% versus 5% once weekly. Clin Exp Dermatol. 1992;17(Suppl 1):41–43.
56. Baran R, Tosti A, Hartmane I, et al. An innovative water-soluble biopolymer improves efficacy of ciclopirox nail lacquer in the management of onychomycosis. J Eur Acad Dermatol Venereol. 2009;23:773–781.
57. Elewski BE, Rich P, Pollak R, et al. Efinaconazole 10% solution in the treatment of toenail onychomycosis: two phase 3 multicenter, randomized, double-blind studies. J Am Acad Dermatol. 2013;68:600–608.
58. Bhatt V, Sarpotdar P, Pillai R, et al. Development of an optimal formulation for efinaconazole a novel antifungal agent for the treatment of onychomycosis by topical application. Poster presented at 71st Annual Meeting, American Academy of Dermatology; Miami Beach FL; 2013.
59. Sugiura K, Hosaka S, Arakawa Y, et al. Unique properties of efinaconazole 10% solution, a new topical treatment for onychomycosis. Poster presented at 71st Annual Meeting, American Academy of Dermatology; Miami Beach FL; 2013.
60. Jo Siu WJ, Tatsumi Y, Senda H, et al. Comparison of in vitro antifungal activities of efinaconazole and currently available antifungal agents against a variety of pathogenic fungi associated with onychomycosis. Antimicrob Agents Chemother. 2013;57(4):1610–1616.
61. Tatsumi Y, Yokoo M, Senda H, Kakehi K. Therapeutic efficacy of topically applied KP-103 against experiemtal tiena ungalum in guinea pigs in comparison with amorolfine and terbinafine. Antimicrob Agents Chemother. 2002;46:3797–3801.
62. Hashiguchi T, Kodama A, Ryu A, et al. Retention capacity of topical imidazole antifungal agents in the skin. Int J Pharm. 1998;161(2):195–204.
63. Murthy NS, Wiskirchen DE, Bowers CP. Iontophoretic drug delivery across human nail. J Pharm Sci. 2007;96(2):305–311.
64. Alley MRK, Baker SJ, Beutner KR, et al. Recent progress in the topical therapy of onychomycosis. Expert Opin Investig Drugs. 2007;16(2):157–167.
65. Gupta AK, Fleckman P, Baran R. Ciclopirox nail lacquer topical solution 8% in the treatment of toenail onychomycosis. J Am Acad Dermatol. 2000;43:S70–S80