Grace K. Kim, DO; James Q. Del Rosso, DO, FAOCD
Dr. Kim is Dermatology Research Fellow, Mohave Skin & Cancer Clinics, Las Vegas, Nevada. Dr. Del Rosso is Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada. Disclosure: Drs. Kim and Del Rosso report no relevant conflicts of interest.
Tendinopathy induced by fluoroquinolone (FQ) antibiotics is a topic of controversy, with many researchers believing in a direct causal relationship while others believing that the risk is negligible. With the advent of a “black-box warning” mandated by the United States Food and Drug Administration (FDA), there is enough data to suggest that FQs should be used cautiously in a selected population of patients.[1] This review is designed to unveil for the clinician the pathophysiology, epidemiology, treatment options, and outcomes related to FQ-induced tendinitis and tendon rupture.
How was fluoroquinolone-induced tendinopathy originally recognized?
The first published report of Achilles tendinopathy associated with FQs was published in New Zealand in 1983.[2] In this case, a 56-year-old renal transplant patient was treated with norfloxacin for a urinary tract infection and septicemia. Subsequently, there have been many other anecdotal case reports and case-controlled studies reporting similar findings, most of them originating from France.[3–5] FQs are a popular class of antibiotics with broad-spectrum coverage including several Gram-negative pathogens.[2] High oral bioavailability with extensive tissue penetration support the use of FQ antibiotics for a wide variety of bacterial infections, with the mode of excretion being predominantly renal.[2] FQs are commonly prescribed to adults treated on an outpatient basis for community-acquired infections involving the respiratory, urogenital, and gastrointestinal tracts.6 FQs exhibit a high affinity for connective tissue with concentrations in the bone and cartilage that exceed those measured in serum, making them ideal for joint and bone infections.[7] Achilles tendinitis or rupture is among the most serious side effects associated with FQ use, with reports markedly increasing, especially with ciprofloxacin, a very popular FQ used orally in the ambulatory setting.[8]
Which FQs have been associated with tendinopathy/tendon rupture?
In a World Health Organization (WHO) survey in Australia of tendon disorders associated with FQ use, ciprofloxacin was found to be the causal agent in 90 percent of cases, with the risk of tendinopathy appearing to be dose independent.[9–10]
Additional reports have also been noted with norfloxacin, pefloxacin, ofloxacin, and recently levofloxacin as precipitating agents.6 The large body of data provided by clinical reports, histopathological examination, and experimental studies provides cogent evidence supporting a direct link between FQ use and tendonitis/tendon rupture.[6] As of July 2008, the FDA mandated that all FQ products have a black-box warning indicating an increased risk in adverse events including tendon rupture. FQ products affected by the labeling changes include ciprofloxacin (Cipro, Bayer, and generics), extended-release ciprofloxacin (Cipro XR, Bayer; Proquin XR, Depomed), gemifloxacin (Factive, Oscient), levofloxacin (Levaquin, Ortho McNeil), moxifloxacin (Avelox, Bayer), norfloxacin (Noroxin, Merck), and ofloxacin (Floxin, Ortho McNeil, and generic).[1]
What are the risk factors associated with FQ-induced tendinopathy/tendon rupture?
Risk factors associated with FQ-induced tendon disorders include age greater than 60 years, corticosteroid therapy, renal failure, diabetes mellitus, and a history of musculoskeletal disorders.[11] Further details on risk factors associated with FQ use are discussed below.
What FQ agents other than ciprofloxacin have been reported to predispose patients to tendinopathy/tendon rupture?
According to past epidemiological studies, pefloxacin and ofloxacin were frequently associated with tendon disorders based on case reports.[12,13] Overall, ofloxacin appears to exhibit a stronger association.[14–17]
What basic information is known about Achilles tendinopathy?
Achilles tendinopathy is considered an overuse syndrome from excessive loading of the tendon during vigorous training activity.[11] Possible mechanical causes include poor gastrocnemius-soleus flexibility, low-flexibility shoes, muscle fatigue resulting in tendon elongation, and micro-tearing.[11] Achilles tendon rupture (ATR) is a condition that manifests as a complete or partial rupture of the Achilles tendon.[3]
The prevalence of ATR has been reported in a number of studies with a range of 6 to 37/100,000 persons and increases with age.[18] There is a peak incidence of ATR in middle-aged individuals due to weakening of the tendon from a decline in physical activity, although rheumatoid arthritis, male gender (2:1), and use of corticosteroids are additional risk factors.[18] Exposure to corticosteroids, both systemic and with local application, has been reported to be a common antecedent of ATR and is thought to increase risk of rupture through tendon atrophy and weakening.[19–23] The combination of corticosteroid use, renal failure, and FQ use has been associated with ATR up to one year after FQ antibiotic exposure.[5] Achilles tendonitis precedes acute rupture when associated with FQ-induced tendinopathy.[24] Although most young individuals recover completely following tendon rupture, ATR can be associated with considerable morbidity and loss of function, especially among the elderly, thus emphasizing the importance of assessing for risk factors and recognizing early symptoms of tendinitis.[24–26]
What adverse events are associated with FQ use?
The most common adverse effects associated with FQ use are gastrointestinal (1–7%), neurological (0.1–0.3%), cutaneous eruptions (0.5–2.5%), gait disturbances (<1%), elevation of serum transaminases (1.8–2.5%), and hematological abnormalities (very rare).[27] These side effects associated with fluoroquinolones are infrequent (usually 4–8%), overall minor or mild in severity (1–2.8% requiring cessation of treatment), dose dependent, and reversible.[27]
What epidemiological and clinical data are available about FQ-induced tendinopathy including tendon rupture?
FQ-induced tendinopathy has been observed at various dosages, with the most profound effects at higher dosages.[28] The average age of FQ-induced tendinopathy is 64 years, with a male-to-female ratio of 2:1, and a 27-percent incidence of bilateral involvement.[6] Although more than 95 percent of cases of tendinitis/rupture secondary to FQ involve the Achilles tendon, other reported sites of tendon involvement include the quadriceps, peroneus brevis, and rotator cuff.[29] Although there is no definitive explanation as to why drug-induced tendinopathy/rupture most frequently involves the Achilles tendon, it has been theorized that the rapid and immense loading during weight-bearing activities (i.e., walking, running, athletic activities) may place the Achilles tendon at greater risk than other tendon sites.[12] Based on epidemiological data, when compared to other classes of antibiotics, FQs demonstrate a 3.8-fold greater risk for development of Achilles tendinitis/rupture.[30] In addition, in a large population-based case control analysis, patients treated with FQs exhibited a substantially increased risk of developing tendon disorders overall (1.7-fold), tendon rupture (1.3-fold), and ATR (4.1-fold).[3] In the same study, compared to age-matched controls, patients taking FQs with concurrent exposure to corticosteroids were found to experience a compounding effect on the risk of tendon rupture, specifically a 46-fold greater predisposition.[3] Age also appears to correlate with a greater risk of FQ-induced tendinopathy. It has been estimated that 2 to 6 percent of all ATRs among patients greater than 60 years of age could be attributed to the use of a FQ.[16] Additionally, patients greater than 60 years of age who were recently treated with a FQ for 1 to 30 days were at a 1.5-fold and a 2.7-fold greater risk for development of tendon disorders and tendon rupture as compared to patients less than 60 years of age, respectively.[31] Some authors have recommended that patients with a history of Achilles tendinitis and advanced age should not be prescribed FQ antibiotics.[32] Although the prevalence of FQ-induced tendon injury is low in the general population (0.14–0.4%), the risk of tendinitis/tendon rupture is substantially increased in patients with chronic renal failure, hemodialysis, and systemic corticosteroid therapy.[31,33–37] Decreased renal clearance of FQ may also play a contributory role in predisposing patients to tendinopathies.[33] In addition, according to the FDA safety information and adverse event reporting program, kidney, heart, and lung transplant recipients are at an increased risk for development of tendinopathies associated with FQ use.[1] Obesity, hyperlipidemia, hyperparathyroidism, musculoskeletal disorders, and diabetes are all well-established risk factors for tendinopathy/tendon rupture, and with their risk potential possibly exacerbated by concurrent FQ exposure.[3]
What is the latency period between the onset of FQ exposure and development of tendinopathy/tendon rupture?
The mean latency period between the start of FQ treatment and occurrence of tendinopathy has been reported to be a few hours to months, with a median onset of 6 days.[3] In one report, half of tendon ruptures occurred within one week of FQ administration, with symptoms starting within two hours in one patient.[6] Approximately 85 percent of patients present in less than one month, with 20 percent having a history of oral corticosteroid use.6 Available data indicates that the risk of a person suffering an ATR was three-fold higher within 90 days of using a FQ for the first time.[38] Approximately 41 to 50 percent of patients with FQ-induced tendinopathy experienced ATR even after FQ therapy was discontinued.[4,15]
What is the suggested pathophysiology of FQ-induced tendinopathy/tendon rupture?
The exact pathophysiology of FQ-induced tendinopathy remains elusive; however, some concepts have been suggested. FQs are synthetic antibiotics that act by inhibiting bacterial DNA gyrase (topoisomerase II).[27] DNA gyrase is directly involved in DNA replication and cell division.10 Theoretically, FQs should not exert a negative effect on human cell lines because the affected bacterial enzymes have little homology with mammalian DNA gyrase.[10] However, it is possible that FQs have a direct cytotoxic effect on enzymes found in mammalian musculoskeletal tissue.[10] Because animal studies have shown that FQs may damage juvenile weight-bearing joints, most FQs are contraindicated in children and during pregnancy and lactation.[39–40] FQs have chelating properties against several metal ions (e.g., calcium, magnesium, aluminum), and have been known to cause direct toxicity to type 1 collagen synthesis and promote collagen degradation.[33,35] Experiments on immature laboratory animals (dogs, rabbits, and rats) have shown that FQs cause cartilage damage by inducing necrosis of chondrocytes (36 hours after treatment), disruption of the extracellular matrix, and formation of vesicles and fissures at the articular surface.[41] In-vitro studies in cultured tendon cells have confirmed the clinical observation that FQs can increase the risk of tendon rupture.[42] Under normal circumstances, the rate of matrix turn-over and tendon fibroblast is low.[10]
Other precipitating factors, such as age and corticosteroid use, do not allow the tendon to repair adequately, resulting in irreversible matrix alteration.[43] It has been theorized that FQs disproportionately affect human tendons that have a limited capacity for repair, such as in older patients or structural compromise (i.e., pre-existing tendinopathy or trauma).[10]
What are the clinical manifestations of FQ-induced tendinopathy/tendon rupture?
The Achilles tendon is most commonly affected in FQ-induced tendinopathy, occurring in 89.8 percent of cases; however, other tendons, such as biceps brachii, supraspinatus, and extensor pollicis longus, can also be affected.[11] Other sites included the triceps epicondyle, flexor tendon sheath, patellar tendon, quadriceps muscle, rotator cuff, and subscapularis terrea.[33] Up to 50 percent of cases may present with bilateral involvement.[44] Depending on the degree of involvement of the joint, patients may experience pain, swelling, or inflammation in the tendon area for up to two weeks before rupture occurs.[1] Signs of tendon rupture can include a “snap” or “pop“ in the area, bruising, or immobility of the joint.[1] Tendon rupture is almost always preceded by spontaneous pain at the bony insertion 2 to 3cm above the insertion point, believed to be correlated with diminished vascularization at this anatomic site.[27] FQ-induced tendinitis is distinguished from other forms of tendinopathy by both the abrupt onset and sharp pain that occur spontaneously upon walking or palpation.[27] With Achilles involvement, patients can experience difficulty to perform plantar flexion of the foot (Thompson’s sign).[27]
What histological findings have been found in cases of FQ-induced tendinopathy?
Histologically, interstitial edema and severe degenerative changes with absence of an inflammatory infiltrate are seen in FQ-induced tendinopathy, findings which have also been observed in overuse conditions in athletes.[11] Chondrocyte depletion and fissures on adjacent nonruptured tendons are also suggestive of direct toxicity related to FQ exposure.[6] Importantly, these findings lack specificity and closely resemble those found with idiopathic tendon ruptures.[27] In one study, FQ-induced Achilles tendinopathy showed necrosis and cystic changes that are not found in nondrug-associated tendinopathies.[45] Because histopathological findings are similar to those observed in overuse conditions in athletes, support is given to the theory that FQs alter cellular function and create a change in the cell-to-matrix ratio.[36]
Are any radiological imaging procedures helpful in assessing FQ-induced tendinopathy/tendon rupture?
Both ultrasound and magnetic radiographic imaging (MRI) can provide information on the morphology of tendons and their surrounding structures. These imaging procedures are useful in evaluating the various stages of degeneration, which helps in differentiating between peritendinitis and tendinosis.[11] Although the role of plain radiography is limited in assessing soft tissue injury such as tendinopathy, the presence or absence of a fracture can be evaluated in this manner. Ultrasonography is relatively inexpensive and is a readily available imaging method that can be used to confirm partial or complete tendon rupture.[27] Hypoechoic areas, consistent with degenerative tissue, and increased tendon thickness are important findings on ultrasound.[11] Findings of acute tears include gaps at the site of rupture, hyperemic torn tendon ends, and fluid collection around the rupture site.[11] MRI is also useful in identifying tendinopathy and can provide more precise information about the extent of involvement.[27] Consistent with tendinosis, an MRI may also show extensive thickening of the tendons from insertion to the musculotendinous junction.[11] Importantly, patients who are asymptomatic may also exhibit MRI abnormalities corresponding to edema secondary to ischemia.[27]
What is the management of FQ-induced tendinopathy/tendon rupture?
After identifying the severity of involvement in a case of tendinopathy induced by a FQ antibiotic, treatment should include rest and decreasing the physical load on the tendon.[46] Treatment with a FQ should be discontinued and physical therapy initiated.[44] During the first month of rehabilitation of an Achilles tendinopathy, the affected tendon should be protected with a heel lift, counterforce bracing, and crutches to decrease the tensile load transmitted to the Achilles tendon during walking for six weeks to six months.[47] Approximately 50 percent of patients will recover within 30 days, with 25 percent of patients having symptoms persistent for longer than two months.[4,48] In certain instances, strict bed rest with an attendant, especially in the elderly, may be required.[27] Because rupture can occur even late in the course of treatment or after discontinuation of FQ use, patients receiving a FQ should be counseled to seek medical attention immediately if symptoms, such as redness, pain, swelling, and stiffness, develop.[44] Tendinosis usually recovers over a time course of weeks, usually within two months, after cessation of FQ therapy.[11]
Early diagnosis based on recognition of symptoms suggestive of tendinopathy, followed by FQ discontinuation and supportive treatment, may prevent tendon rupture and tendinitis.[44] In cases of FQ-induced tendon rupture, orthopedic treatment should proceed, as in other cases of tendon disruption, with consideration given to operative therapy after assessing the potential risks versus anticipated benefits of surgical intervention.[27]
What conclusions can be drawn from the available data on FQ-induced tendinopathy/tendon rupture?
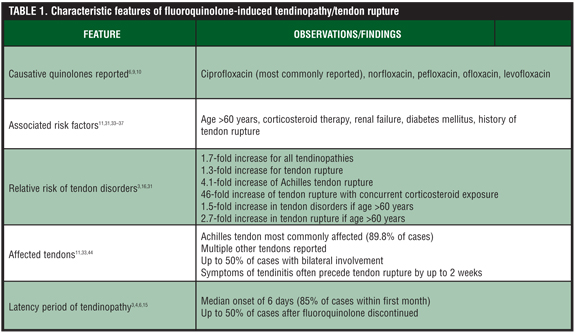
FQs should be used cautiously in patients with risk factors associated with tendinitis, such as advanced age, history of tendon rupture, corticosteroid use, and/or acute or chronic renal dysfunction.[44] A summary of the characteristic features of FQ-induced tendinopathy/tendon rupture is depicted in Table 1.
{kind=link}
Tendinitis can be misdiagnosed as a gouty flare, infection, or venous thrombosis (leg region involvement).[44] Since Achilles tendinitis can be debilitating and may lead to rupture, clinicians may need to monitor changes in gait and for symptoms suggestive of tendinopathy in patients on FQ therapy.[44] Although Achilles tendinopathy is generally the result of repetitive injury, it is useful to keep in mind the possibility of unusual causes such as drug-induced tendinosis and tear.[11] The modalities of ultrasound and MRI are valuable in assessing the presence, extent, and severity of tendon involvement if symptoms and signs of tendinopathy develop.[11] From a clinical perspective it can be difficult to prove a cause-and-effect relationship between a medication and a side effect. This is true concerning tendon rupture, which may occur in the absence of a causative medication, particularly since reported cases frequently had coexisting risk factors. However, the multitude of clinical reports, pathological findings, and experimental models collectively support a strong correlation between FQ use and tendinopathy. In conclusion, whether a FQ antibiotic is the appropriate drug to prescribe is ultimately a decision that the clinician must make depending on the cause and type of infection, the presence or absence of patient-specific risk factors, and the clinically relevant alternatives that are available.
References
1. Waknine Y. Fluoroquinolones earn black box warning for tendon related adverse effects. www.emedicine. medscape.com.
2. Bailey RR, Kirk JA, Peddie BA. Norfloxacin induced rheumatoid disease. N Z Med J. 1983;96:590.
3. Giovanni C, Zambon A, Bertu L, et al. Evidence of tendinitis provoked by fluoroquinolone treatment. Drug Saf. 2006;29(10):889–896.
4. Royer RJ, Pierfitte C, Netter P. Features of tendon disorders with fluoroquinolones. Therapie. 1994; 49:75–76.
5. Pierfitte C, Gillet P, Royer RJ. More on fluoroquinolone antibiotics and tendon rupture [letter]. N Engl J Med. 1995;332(3):193.
6. Akali AU, Niranjan NS. Management of bilateral Achilles tendon rupture associated with ciprofloxacin: a review and case presentation. J Plast Reconstr Aesthet Surg. 2008;61(7): 830–834.
7. Melhus A, Apelqvist J, Larsson J, et al. Levofloxacin-associated Achilles tendon rupture and tendinopathy. Scand J Infect Dis. 2003;35(10): 768–770.
8. Gultuna S, Koklu S, Arhan M, et al. Ciprofloxain induced tnedinitis. J Clin Rheumtol. 2009;15(4):201–202.
9. World Health Organization. Pharmaceutical Newsletter. www.who.int/medicines/publications/newsletter/en/news2003_1.pdf.
10. Williams RJ, Attia E, Wickiewicz TL. The effect of ciprofloxacin on tendon, paratenon, and capsular fibroblast metabolism. Am J Sports Med. 2000;28(3);364–369.
11. Yu C, Guiffre BM. Achilles tendin-opathy after treatment with fluoro-quinolone. Australas Radiol. 2005; 49:407–410.
12. Ribard P, Audisio F, Kahan MF, et al. Seven Achilles tendinitis including 3 complicated by rupture during fluoroquinolone therapy. J Rheumatol. 1992;19(9):1479–1481.
13. Meyboom RH, Olsson S, Knol A, et al. Achilles tendinitis induced by pefloxacin and other fluoroquinolone derivatives. Pharmacoepidemiol Drug Saf. 1994;3:185–189.
14. Van der Linden PD, Puijenbroek EPV, Feenstra J, et al. Tendon disorders attributed to fluoroquinolones: a study on 42 spontaneous reports in the period 1988 to 1998. Arthritis Rheum. 2001;45(3):235–239.
15. Van der Linden PD, Van der Lei J, Nab HW, et al. Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol. 1999;48:433–437.
16. Van der Linden PD, Sturkenboom MC, Herings RM, et al. Increased risk of Achilles tendon rupture with quinolone antibacterial use, especially in the elderly patients taking oral corticosteroids. Arch Intern Med. 2003;163:1801–1807.
17. Wilton LV, Pearce GL, Mann RD. A comparison of ciprofloxacin, nor-floxacin, ofloxacin, azithromycin and cefixime examined by observational cohort studies. Br J Clin Pharmacol. 1996;41:227–284.
18. Seeger JD, West WA, Fife D, et al. Achilles tendon rupture and its association with fluoroquinolone antibiotics and other potential risk factors in a managed care pop-ulation. Pharmacoepidemiol Drug Saf. 2006;15(11):784–792.
19. Dickey W, Patterson V. Bilateral Achilles tendon rupture simulating peripheral neuropathy: unusual complication of steroid therapy. J R Soc Med. 1987;80(6):386–387.
20. Hersh BL, Heath NS. Achilles tendon rupture as a result of oral steroid therapy. J Am Podiatr Med Assoc. 2002;92(6):355–358.
21. Newnham DM, Douglas JG, Legge JS, Friend JA. Achilles tendon rupture: an underrated complication of corticosteroid treatment. Thorax. 1991;46(11):853–854.
22. Ford LT, DeBender J. Tendon rupture after local steroid injection. South Med J. 1979;72(7):827–830.
23. Kleinman M, Gross AE. Achilles tendon rupture following steroid injection. J Bone Joint Surg Am. 1983;65(9):1345–1347.
24. Royer RJ. Adverse drug reactions with fluroquinolones. Therapie. 1996;51:419–420.
25. Le Huec JC, Schaeverbeke T, Chauveaux D, et al. Epidondylitis after treatment with fluoroquinolone antibiotics. J Bone Joint Surg Br. 1995;77:293–295.
26. McGarvey WC, Singh D, Trevino SG. Partial Achilles tendon ruptures associated with fluoroquinolone antibiotics: a case report and literature review. Foot Ankle Int. 1996;17:496–498.
27. Zavraniecki L, Negrier I, Vergne P, et al. Fluoroquinolone induced tendinopathy: report of 6 cases. J Rheumatol. 1996;23:516–520.
28. Movin T, Gad A, Gunter P, et al. Pathology of the Achilles tendon in association with ciprofloxacin treat-ment. Foot Ankle Int. 1997;18: 297–299.
29. Casparian JM, Luchi M, Moffat RE, et al. Quinolones and tendon ruptures. South Med J. 2000;93:488–491.
30. Chlajed PN, Plit ML, Hopkins PM, et al. Achilles tendon disease in lung transplant recipients: association with ciprofloxacin. Eur Respir J. 2002;19(3):469–471.
31. Corrao G, Zambon A, Bertù L, et al. Evidence of tendinitis provoked by fluoroquinolone treatment: a case-control study. Drug Saf. 2006; 29(10):889–896.
32. Muzi F, Gravante G, Tati E, Tate G. Fluoroquinolones-induced tendonitis and tendon rupture in kidney transplant recipients: 2 cases and a review of the literature. Transplant Proc. 2007;39:1673–1675.
33. Khaliq Y, Zhanel GG. Fluoroquinolone-associated tendinopathy: a critical review of the literature. Clin Infect Dis. 2003;36:1404–1410.
34. Yu C, Giuffre BM. Achilles tendinopathy after treatment with fluoroquinolone. Australas Radiol. 2005;49:407–410.
35. Van der Linden PD, Van Puijenbroek EP, Feenstra J, et al. Tendon disorders attributed to fluoroquinolones: a study on 42 spontaneous reports in the period 1988 to 1998. Arthritis Rheum. 2001;45:235–239.
36. Marti HP, Stoller R, Frey FJ. Fluoroquinolones as a cause of tendon disorders in patients with renal failure/renal transplants. Br J Rheumatol. 1998;37(3):343–344.
37. Haddow LJ, Chandra SM, Hajela V, et al. Spontaneous Achilles tendon rupture in patients treated with levofloxacin. J Antimicrob Chemother. 2003;51(3):747–748.
38. Sode J, Obel N, Hallas J, et al. Use of fluoroquinolone and risk of Achilles tendon rupture: a population-based cohort study. Eur J Clin Pharmacol. 2007;63(5):499–503.
39. Hayem G, Carbon C. A reappraisal of quinolone tolerability: the experience of their musculoskeletal adverse effects. Drug Saf. 1995;13(6):338–342.
40. Ribard P, Kahn MF. Rheumatological side-effects of quinolones. Baillieres Clin Rheumatol. 1991;5(1):175–191.
41. Burkhardt JE, Hill MA, Carlton WW. Morphologic and biochemical changes in articular cartilages of immature beagle dogs dosed with difloxacin. Toxicol Pathol. 1992;20: 246–252.
42. Kempka G, Ahr HJ, Ruther W, et al. Effects of fluoroquinolones and glucocorticoids on cultivated tendon cells in vitro. Toxicol In Vitro. 1996;10:743–754.
43. Van den Berg WB, Kruijen MM, Van de Putte LA. The mouse patella assay: an easy method of quantitaing articular cartilage chondrocyte function in vivo and in vitro. Rheumatol Int. 1982;1:165–169.
44. Damuth E, Heidelbaugh J, Malani PN, Cinti SK. An elderly patient with fluoroquinolone-associated Achilles tenditis. Am J Geriatr Pharmacother. 2008;6(5):264–268.
45. Petersen W, Laprell H. [Insidious rupture of the Achilles tendon after ciprofloxacin-induced tendopathy. A case report]. Unfallchirurg. 1998: 101:731–734.
46. Huston KA. Achilles tendinitis and tendon rupture due to fluoroquinolone antibiotics. N Engl J Med. 1994;331: 748.
47. Greene BL. Physical therapist management of fluoroquinolone-induced Achilles tendinopathy. Physical Therapy. Phys Ther. 2002;82(12):1224–1231.
48. McGarvey WC, Singh D, Trevino SG. Partial Achilles tendon ruptures associated with fluoroquinolone antibiotics: a case report and literature review. Foot Ankle Int. 1996;17: 496–498.