Dailana Louvain Marinho Costa, MD; Heloisa Helena Moura; Rosangela Rodrigues;
Juan Pineiro-Maceira, MD, PhD; Marcia Ramos-e-Silva, MD, PhD
Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
Disclosure: The authors report no relevant conflicts of interest.Abstract
The authors present a case of telangiectasia macularis eruptiva perstans, an uncommon form of cutaneous mastocytosis, in a 53-year-old man and discuss its clinics, pathophysiology, laboratory results, and treatment. Cutaneous mastocytosis is a proliferation of masts cells on the skin without involvement of other organs. Typically the lesions of telangiectasia macularis eruptiva perstans are telangiectatic macules with color ranging from light to dark brown. It is more frequent in adults, with some reports in children. It is usually insidious, without symptoms at the beginning and, although a manifestation of cutaneous mastocytosis, telangiectasia macularis eruptiva perstans may present systemic involvement. It is very important for dermatologists to know this form of cutaneous mastocytosis and to make an early diagnosis, so they may treat the disorder and improve their patients’ quality of life. (J Clin Aesthet Dermatol. 2011;4(10):52–54.)
Telangiectasia macularis eruptiva perstans (TMEP), described by Parkes Weber in 1930, represents a rare form of mastocytosis. The typical lesions are telangiectatic macules with background color ranging from light to dark brown. TMEP develops more frequently in adults, although there are reports of cases affecting children.[1–6]
Despite most cases being limited to the skin, with lesions on the chest and extremities, systemic involvement may occur. Bone marrow, gastrointestinal tract, liver, spleen, and lymph node involvement are not uncommon. Hematological abnormalities may also be present and the association with multiple myeloma and polycythemia vera has been reported.[7] Histologically, the lesions are characterized by an infiltrate consisting of mast cells around venules and dilated capillaries of the superficial venous plexus of the dermis.[1] The treatment is based on the symptoms presented by the patient, and there is no gold standard treatment to date.[1,7,8]
CASE REPORT
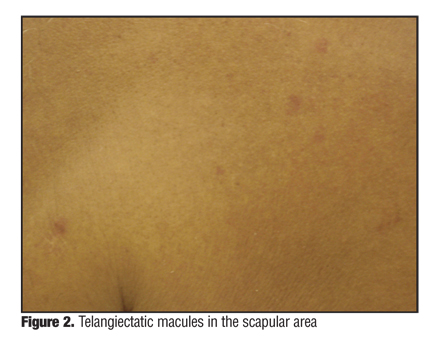
A 53-year-old man presented with asymptomatic cutaneous lesions (Figure 1 and Figure 2). He stated that the lesions evolved over a period of three years. He denied systemic symptoms and/or aggravating factors and was monitored for hypertension and dyslipidemia.
{kind=link}
{kind=link}
Facial and upper chest erythema was observed on examination, as were small erythematous macules with telangiectasia on the surface measuring about 0.5cm located in the upper limbs and chest. They became slightly papular upon friction. There was no hepatosplenomegaly and palpable lymph nodes.
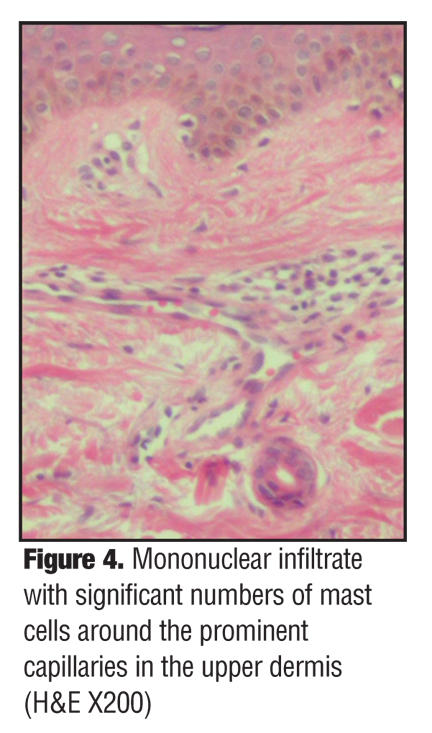
The biopsy of the skin lesion showed a mononuclear infiltrate with the presence of significant numbers of mast cells around the capillaries prominent in the upper dermis (Figure 3 and Figure 4). The remaining laboratory tests, which included complete blood count, peripheral blood film examination, and liver function tests, were all within normal limits. A liver biopsy was not performed because laboratory exams and physical examination were normal.
{kind=link}
{kind=link}
The suggestive clinical picture and the typical histopathology exam confirmed the diagnosis of telangiectasia macularis eruptiva perstans. As the patient had no clinical symptoms, no medication was administered, and he was monitored periodically by a general practitioner and a dermatologist.
DISCUSSION
Cutaneous mastocytosis is the proliferation of mast cells in the skin without any evidence of involvement of other organs. TMEP, unlike other forms of cutaneous mastocytosis, affects mainly young adults. The clinical picture is characterized by brownish erythematous macules, telangiectasia, irregular borders, and a diameter between 2 and 6mm. The usual location of the lesions is in the chest and limbs. Darier’s sign is absent in most cases.[1,5,7,9] Symptoms can be only cutaneous or only systemic, depending if there is local or generalized release of mediators from mast cells. Mast cells can infiltrate multiple organs, including skin, spleen, bone marrow, liver, and lymph nodes, with the skin being the most frequent target.
Cutaneous mastocytosis is associated with local and systemic symptoms, including cutaneous flushing; blisters; dyspnea; rash; exacerbation of asthma; hypotension; gastrointestinal disorders, such as gastroesophageal reflux; ulcers; and diarrhea. These symptoms result from mast cell degranulation with the release of several mediators, histamine being the most significant of all mediators, which can cause both local and systemic reactions.[10]
Most cases of cutaneous mastocytosis start in childhood. TMEP is a rare form, occurring more often in adults than children. The age of manifestation has an important value for prognosis. Most pediatric patients with cutaneous mastocytosis show improvement in symptoms over time, with 50 percent showing resolution of symptoms in adolescence and only 10 to 15 percent persisting in adulthood.[10]
In pediatric patients, unlike in adults, it is believed that a transitory deregulation of growth factors occurs. In adults, a c-kit proto-oncogene mutation is observed, which entails a mast cell hyperplasia. The c-kit encodes the KIT proto-oncogene, a tyrosine kinase, which is the mast cell’s growth factor receptor. This particular mutation, however, was not found in pediatric patients or familial mastocytosis.[8,11] Although the c-kit mutations are not found in all patients with cutaneous mastocytosis, proto-oncogene alterations may indicate a more aggressive behavior of the mastocytosis.
Cutaneous mastocytosis may appear in four clinical variants: urticaria pigmentosa, isolated mastocytoma, cutaneous diffuse or erythrodermic mastocytosis, and telangiectasia macularis eruptiva perstans. The occurrence of systemic symptoms may indicate the presence of associated hematological diseases or even a systemic mastocytosis condition. Signs of systemic involvement include hepatosplenomegaly, lymphadenopathy, and bone alterations.[9]
Although TMEP is a manifestation of cutaneous mastocytosis, systemic involvement may occur. High tryptase serum levels may be an indicator of systemic involvement. In a study with 52 patients, the prevalence of bone marrow biopsy samples compatible with systemic mastocytosis increased, following the same proportion of the total tryptase level. The biopsy specimens were 100-percent positive when the total tryptase was greater than 75ng/mL and 50-percent positive when total tryptase levels were 20 to 75ng/mL.[8]
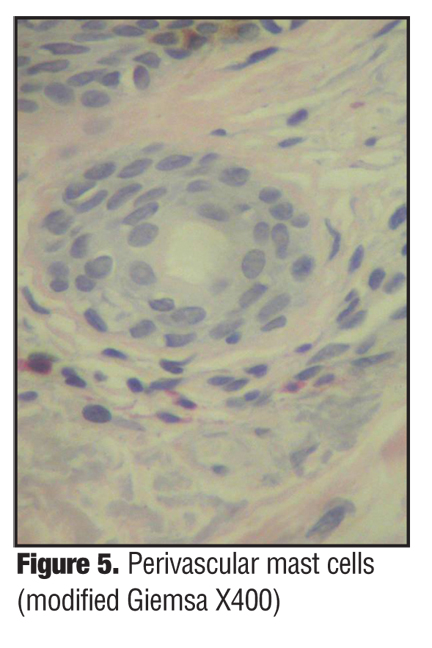
Histologically, TMEP is characterized by a small mononuclear infiltrate, containing significant numbers of mast cells around the superficial venous plexus capillaries. Special stains, such as Giemsa or toluidine blue, help to highlight the presence of mast cells, revealing their metachromatic cytoplasmic granules[6,7,9] and are very useful in the diagnostic evaluation (Figure 5). Dermoscopy of TMEP lesions shows linear spots arranged in a reticular pattern.[12]
{kind=link}
The treatment of patients with TMEP depends on the presence of systemic involvement or clinical symptoms. There is no gold standard medication for the treatment of TMEP and it is essential to identify and avoid factors that stimulate the mast cell’s degradation, such as exposure to sunlight, extreme temperatures, alcohol, and drugs. H1 antagonists are used to control pruritus and urticaria. Psoralen plus ultraviolet light A treatment results in improvement of symptoms and regression of skin lesions by inhibiting histamine release by mast cells. However, recurrence can occur after a variable interval from the end of treatment. The intense light pulsed with a 585nm wavelength has shown efficiency in two cases reported in the literature, but with recurrence after 14 months of treatment. Ketotifen, doxepin, cromolyn sodium, topical and systemic corticosteroids, leukotriene antagonists, alpha interferon, and use of “electron beam” radiation were also reported.[1,7,8,9]
CONCLUSION
Although sometimes insidious and without symptoms at the beginning, TMEP is a rare form of mastocytosis seen typically in adults. Dermatologists must be aware of this condition, so the diagnosis can be made at an early stage, improving the patient’s quality of life.
References
1. Soter NA. The skin in mastocytosis. J Invest Dermatol. 1991;96(3 Suppl):32S–39S.
2. Soter NA. Mastocytosis and the skin. Hematol Oncol Clin North Am. 2000;14(3):537–555.
3. Kalayciyan AK, Koto€yan A. Telangiectasia macularis eruptiva perstans. J Eur Acad Dermatol Venereol. 2001;15(3):263–264.
4. Rishpon A, Matz H, Gat A, Brenner S. Telangiectasia macularis eruptiva perstans: unusual presentation and treatment. Skinmed. 2006;5(6):300–302.
5. Sarkany RP, Monk BE, Handfield-Jones SE. Telangiectasia macularis eruptiva perstans: a case report and review of the literature. Clin Exp Dermatol. 1998;23(1):38–39.
6. Gibbs NF, Friedlander SF, Harpster EF. Telangiectasia macularis eruptiva perstans. Pediatr Dermatol. 2000;17(3): 194–197.
7. Sotiriou E, Apalla Z, Ioannides D. Telangiectasia macularis eruptive perstans successfully treated with PUVA therapy. Photodermatol Photoimmunol Photomed. 2010;26(1): 46–47.
8. Nguyen NQ. Telangiectasia macularis eruptiva perstans. Dermatol Online J. 10(3):1.
9. Oliveira CR, Albuquerque GC, Simon EF, Quinete SS, Carvalho SC. Case for diagnosis. Telangiectasia macularis eruptiva perstans. An Bras Dermatol. 2009;84(1):87–89.
10. Briley LD, Phillips CM. Cutaneous mastocytosis: a review focusing on the pediatric population. Clin Pediatr (Phila). 2008;47(8):757–761.
11. Lee HW, Jeong YI, Choi JC, et al. Two cases of telangiectasia macularis eruptiva perstans demonstrated by immuno-histochemistry for c-kit (CD 117). J Dermatol. 2005;32(10): 817–820.
12. Akay BN, Kittler H, Sanli H, Harmankaya K, Anadolu R. Dermatoscopic findings of cutaneous mastocytosis. Dermatology. 2009;218(3):226–230.