
James Q. Del Rosso, DO, FAOCD; Grace K. Kim, DO
Introduction
Seborrheic dermatitis (SD) is a common inflammatory dermatoses that may affect infants, adolescents, and adults of all ethnicities and races.[1,2] SD exhibits two incidence peaks, one during infancy, and the other during the fourth to sixth decades of life.[3] The prevalence of SD ranges from 1 to 5 percent in the immunocompetent population and increases in the immunocompromised population, especially among patients with acquired immunodeficiency syndrome (AIDS).[2–4] Infantile SD occurs between the second and tenth week of life and peaks at three months of age.[4] Infantile SD is distinguished from adult or adolescent SD in that the infantile form is almost always confined to the first 3 to 12 months of life, while adult SD is characteristically chronic and relapsing throughout life.[5] SD can also present in association with other skin disorders, such as atopic dermatitis (AD), which can often create diagnostic confusion. In one study, 49 percent of children with AD between the ages of 2 to 12 months had a history of infantile SD as compared to 17 percent of controls.[4] SD has also been observed in conjunction with other skin diseases, such as rosacea (rosacea-seborrheic dermatitis overlap), blepharitis, acne vulgaris (AV), pityriasis versicolor, and Malassezia folliculitis.[6–9]
Although the pathophysiology of SD is not completely understood, correlation of SD flares with proliferation of Malassezia species (spp) and clinical response of SD to antifungal agents (i.e., ketoconazole, ciclopirox) have led many researchers and clinicians to believe that Malassezia spp play a pivotal role in the pathogenesis of SD.[1,2] SD is viewed as an inflammatory dermatosis similar to AV. In AV, the proliferation of the commensal bacterium Propionibacterium acnes stimulates an immunological cascade, which contributes to the pathogenesis of AV. In SD, proliferation of Malassezia spp, which are commensal yeasts, appears to trigger an immunological response, which stimulates inflammation that precipitates flares of SD, although the inflammatory pathway in SD is not as well defined as with AV.[1,2,4,5]
When does skin become colonized with Malassezia spp?
At birth, neonatal skin is generally sterile; however, resident flora may be detected within the first three hours of life.[10] Factors associated with neonatal colonization includes length of stay in an intensive care department, gestational age, birth weight, use of parenteral nutrition, use of antimicrobial medication, presence of a central venous catheter, surgery along with the presence of a central venous catheter, and surgery along with the presence of a nasogastric tube.[10] Skin colonization with Malassezia spp has been reported to be as high as 13 to 50 percent in the first week of life.[11,12] It has been suggested that exposure to transient flora from the maternal genital tract is the origin of newborn skin colonization.[10] Breast feeding has also been assumed to correlate with skin colonization in newborns.[13] The frequency of bathing, use of skin care products, lubricants, and use of any occlusive agents have all been associated with colonization of infantile skin with Malassezia spp.[13]
At puberty, the increase in sebaceous lipids appears to promote a “friendly environment” for more persistent colonization by Malassezia spp.[2] Malassezia spp are lipophilic yeasts that are normal components of the human adult skin flora.[1,2,4,5] Nine known species have been identified, with seven of them associated with human commensal flora.[1] Investigators have found M. fufur, M. sympodialis, M. obtuse, and M. slooffiae in SD lesions.[14] M. globosa and M. restricta have been identified as the most common organisms associated with SD, predominating in areas such as the scalp in individuals with SD or dandruff.[5,15] Malassezia spp require an exogenous source of specific lipids to grow in culture and tend to appear on skin around the time of puberty, when there is an increase in androgens that cause an elevation in sebum production.[2] Evidence that these yeasts require lipids comes from their ability to produce lipases.[16,17] These lipases are involved in the release of arachidonic acid, which may be involved in cutaneous inflammation.[18]
How are Malassezia spp distributed on human skin?
The distribution of Malassezia spp on the skin is predominantly on the face, scalp, and trunk, all of which are lipid-rich anatomic locations.[2] Importantly, these locations also are sites of predilection for clinical involvement with SD.
What is the relationship between the development of SD and sebum production?
There has been a suggested link between sebum overproduction and Malassezia spp.[2] It has been suggested that Malassezia spp play a role in the pathogenesis of SD due to studies showing isolates of the yeast in affected skin lesions and therapeutic response to antifungal medications, such as ketoconazole and ciclopirox.[5] Nevertheless, patients with SD may have normal sebum production compared to those who have excessive sebum production without SD.[5] Based on individuals who exhibit excessive sebum production without evidence of SD, it is suggested that the amount of sebum production may not be a risk factor for SD development, at least in all affected individuals.[5] It has also been proposed that the composition of skin surface lipids may be a factor in SD development.[5] In patients with SD, triglycerides and cholesterol are elevated; however, squalene and free fatty acids are significantly decreased compared to normal controls.5 Free fatty acids are formed from triglycerides through the action of bacterial lipases produced by P. acnes. Interestingly, P. acnes has been found to be markedly reduced in SD.[5] This suggests that, in SD patients, there may be an imbalance of microbial flora and alterations in the composition of skin surface lipids.[5]
What is the relationship between the cutaneous load of Malassezia spp and SD development?
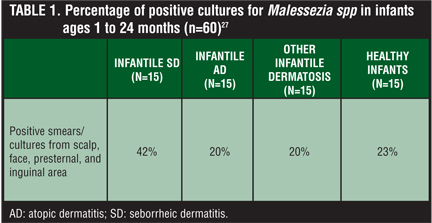
There is evidence suggesting that unaffected skin carries similar loads of Malassezia spp organisms as compared to organism loads observed in SD lesions.[5] Malassezia spp have also been found in both healthy skin and at sites affected with SD (Table 1).[2] It is still controversial whether Malassezia spp organism counts consistently diminish in association with improvement of SD.[1] Additionally, severely immunocompromised human immunodeficiency virus (HIV)-infected patients with SD have been shown not to harbor more organisms compared to yeast counts from the normal population.[5] Nevertheless, some researchers have observed that the number of Malassezia spp organisms drops in correlation with the observed therapeutic benefit after antifungal therapy, and rises again in association with a relapse of SD.[2]
{kind=link}
Some researchers have noted that Malassezia spp are present in high numbers in SD lesions on the scalp.[19,20] There are others that report no significant differences in the number of Malassezia spp organism counts on lesional skin of SD patients compared with nonlesional skin in healthy subjects.[21,22] There are multiple factors that may explain these conflicting results. Malassezia spp are not only restricted to the skin surface, but may be present within layers of the stratum corneum.[23] Malassezia spp organism counts can vary across the full thickness of the stratum corneum, leading to potential variability in the measurement of organism counts depending on the sampling technique used.[18,24]
What other factors have been associated with the development of SD?
Some studies have proposed that the inability to fully metabolize essential fatty acids (EFA) is an underlying mechanism in the pathogenesis of SD.[25] With no consistently observed clear differences in yeast carriage levels noted between healthy and SD patients, it has been suggested that patients with SD might have an immunological predisposition to develop SD, and/or they exhibit a more profound inflammatory response to the organism.[2] It has also been suggested that predisposed individuals demonstrate an altered cutaneous response to the yeasts themselves or to a toxin or byproduct that is produced by Malassezia spp.[2] Inflammation seen in SD may also be irritant in nature owing to the production of toxic metabolites, lipases, and reactive oxygen species by Malassezia spp.[5] There is also additional information suggesting that within lesional skin of SD there is an increase in natural killer 1+, CD16+ cells, which activate complement and increased production of inflammatory interleukins.[26]
What conclusions can be drawn from data regarding the association between Malassezia spp and SD pathogenesis?
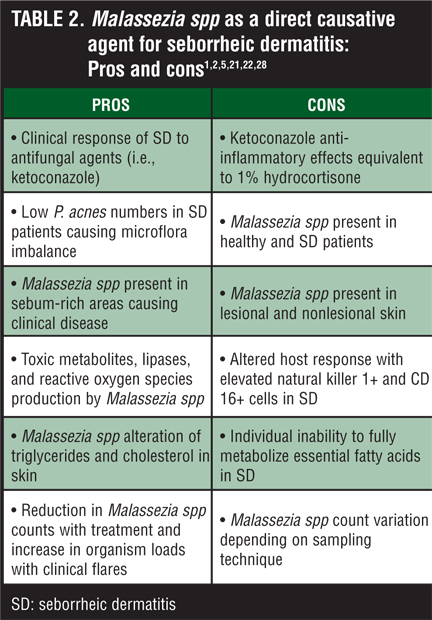
SD is a common inflammatory dermatosis most commonly encountered in adults, although infants and adolescents may be affected. The role of Malassezia spp in the pathogenesis of SD has long been suggested and debated in the literature (Table 2). There are data to suggest that flares of SD are associated with an increase in the organism load of Malassezia spp, and improvement after therapy correlates with a reduction in the organism counts of these yeasts. Other data are not consistent with these findings. There is some suggestion that measurement variability based on different sampling techniques may account for the discrepancies observed among different studies. Additionally, characteristics of skin surface lipids may also be a factor in the development of SD. As appears to be the cases with other inflammatory dermatoses, such as AV, individual susceptibilities and predispositions to inflammatory responses likely play a major role in determining the presence of SD and its severity. Ultimately, the strongest evidence that Malassezia spp play at least a partial role in the development of SD is that significant decreases in the number of these yeasts occur after antifungal treatment of SD and that these decreases correlate with marked visible and symptomatic improvement of SD.
{kind=link}
References
1. Elewski BE. Safe and effective treatment of seborrheic dermatitis. Cutis. 2009;83:333–338.
2. Aditya KG, Bluhm R, Cooper EA, et al. Seborrheic dermatitis. Dermatol Clin. 2003;21:401–412.
3. Poindexter GB, Burkhart CN, Morrell DS. Therapies for pediatric seborrheic dermatitis. Pediatr Ann. 2009;38(6):333–338.
4. Gupta AD, Batra R, Bluhm R et al. Skin disease associated with Malassezia species. J Am Acad Dermatol. 2004;51:785–798.
5. Bolognia JL, Jorizzo JL, Rapini RP, et al. Dermatology. 2nd ed. Spain: Elsevier; 2008.
6. Gupta AK. A random survey concerning aspects of acne rosacea. J Cutan Med Surg. 2001;5:38.
7. McCulley JP, Dougherty JM. Blepharitis associated with acne rosacea and seborrheic dermatitis. Int Ophthalmol Clin. 1985;25:159–172.
8. Faergemann J, Johansson S, Back O. An immunologic and cultural study of Pityrosporum folliculitis. J Am Acad Dermatol. 1986;14:429–433.
9. Sunenshine PJ, Schwartz RA, Janniger CK. Tinea versicolor: an update. Cutis. 1998;61-72.
10. Ayhan M, Sancak B, Karaduman A, et al. Colonization of neonate skin by Malassezia species: relationship with neonatal cephalic pustulosis. J Am Acad Dermatol. 2007;57(6):1012–1018.
11. Ahtonen P, Lehtonen OP, Kero P, et al. Malassezia furfur colonization of neonates in an intensive care unit. Mycoses. 1990;33:543–547.
12. Shattuck KE, Cochran CK, Zabransky RJ, et al. Colonization and infection associated with Malassezia and Candida species in a neonatal unit. J Hosp Infect. 1996;34:123–1239.
13. Bernier V, Weill FX, Hirigoyen V, et al. Skin colonization by Malassezia species in neonates: a prospective study and relationship with neonatal cephalic pustulosis. Arch Dermatol. 2002;138:215–218.
14. Nakabayashi A, Sei Y, Guillot J. Identification of Malassezia species isolated from patients with seborrheic dermatitis, atopic dermatitis, pityriasis versicolor and normal subjects. Med Mycol. 2000;38:337–341.
15. Dawson TL. Malassezia globosa and restricta: breakthrough understanding of the etiology and treatment of dandruff and seborrheic dermatitis through whole-genome analysis. J Investig Dermatol Symp Proc. 2007;12:15–19.
16. Greaves MV, Camp RDR. Prostaglandins, leukotrienes, phospholipase, platelet activating factor and cytokines: an integrated approach to inflammation of human skin. Arch Dermatol Res. 1988;280:S33–S41.
17. Marples RR, Downing DT, Klingman AM. Influence of Pityrosporum species in the generation of free fatty acids in human surface lipid. J Invest Dermatol. 1972;58:155–159.
18. Riciputo RM, Oliveri S, Micali G, et al. Phospholipase activity in Malassezia furfur pathogenic strains. Mycoses. 1996;39:233–235.
19. McGinley KJ, Leyden JJ, Marples RR, et al. Quantitative microbiology of the scalp in non-dandruff, dandruff and seborrheic dermatitis. J Invest Dermatol. 1975;64:401–405.
20. Heng MCY, Henderson CL, Barker DC, et al. Correlation of Pityrosporum ovale density with clinical severity of seborrheic dermatitis as assessed by a simplified technique. J Am Acad Dermatol. 1990;23:82–86.
21. Ashbee HR, Ingham E, Holland KT, et al. The Malassezia furfur serovars A, B, and C in patients with pityriasis versicolor, seborrheic dermatitis and controls. Br J Dermatol. 1993;129:533–540.
22. Bergbrant IM, Faergemann J. Seborrheic dermatitis and Pityrosporum ovale: a cultural and immunological study. Acta Derm Venereol. 1989;69:332–335.
23. Pierard-Franchimont C, Arrese JE, Pieraras GE. Immunohistochemical aspects of the link between Malassezia ovalis and seborrheic dermatitis. J Eur Acad Dermatol Venereol. 1995;4:14–19.
24. Ashbee HR, Evans EGV. Immunology of disease associated with Malassezia species. Clin Microbiol Rev. 2002;15:21–57.
25. Tollesson A, Frith A, Berg A, et al. Essential fatty acids in infantile seborrheic dermatitis. J Am Acad Dermatol. 1993;28:957–961.
26. Faergemann J, Bergbrant IM, Dohse M. Seborrheic dermatitis and Pityrosporum folliculitis: characterization of inflammatory cells and mediators in the skin by immunohistochemistry. Br J Dermatol. 2001;144:549–556.
27. Ruiz-Maldonado R, Lopez-Matinez R, Perez Chavarria L, et al. Pityrosporum ovale in infantile seborrheic dermatitis. Pediatr Dermatol. 1989;6(1):16–20.
28. Van Cutsem J, Van Gerven F, Cauwenbergh G, et al. The anti-inflammatory effects of ketoconazole. J Am Acad Dermatol. 1991;25:257–261.