Amylynne Frankel, MD; Carolin Penrose, MD; Jason Emer, MD
Mount Sinai School of Medicine, Department of Dermatology, New York, New York
Abstract
Cutaneous tuberculosis occurs rarely, despite a high and increasing prevalence of tuberculosis worldwide. Mycobacterium tuberculosis, Mycobacterrium bovis, and the Bacille Calmette-Guérin vaccine can cause tuberculosis involving the skin. Cutaneous tuberculosis can be acquired exogenously or endogenously and present as a multitude of differing clinical morphologies. Diagnosis of these lesions can be difficult, as they resemble many other dermatological conditions that are often primarily considered. Further, microbiological confirmation is poor, despite scientific advances, such as the more frequent use of polymerase chain reaction. The authors report a case that illustrates the challenges faced by dermatologists when considering a diagnosis of cutaneous tuberculosis. (J Clin Aesthetic Dermatol. 2009;2(10):19–27.)
Mycobacterium tuberculosis is a worldwide, problematic, communicable pathogen that has increasingly been regarded as a notable, serious infection in the United States. The underlying basis of this recent epidemic is dependent on such factors as the association of tuberculosis (TB) with the human immunodeficiency virus (HIV) epidemic, increased immigration from endemic countries, and the transmission of TB in crowded settings, such as healthcare facilities, prisons, and homeless shelters.[1–4] Most often TB is an airborne transmissible disease with skin manifestations presenting as a result of hematogenous spread or direct extension from a latent or active foci of infection. However, primary inoculation may occur as a direct introduction of the mycobacterium into the skin or mucosa of a susceptible individual by trauma or injury. Increased risk of acquiring disease occurs with HIV infection, intravenous drug abuse, diabetes mellitus, immunosuppressive therapy, malignancies, end-stage renal disease, and infancy. Cutaneous tuberculosis (CTB) is frequently elusive as it mimics a wide differential diagnosis and also evades microbiological confirmation despite recent advances in sophisticated techniques.[5] Although rare, given its worldwide prevalence, it is important for clinicians to recognize the many clinical variants of CTB to prevent missed or delayed diagnoses.
Case Report
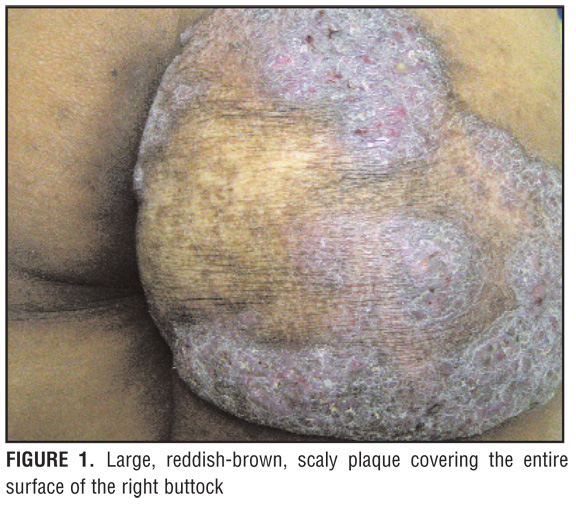
A 24-year-old Hispanic woman presented with a painful lesion on her right buttock that began during her pregnancy four years prior. The lesion appeared as a large, reddish-brown, scaly plaque with well-defined borders and central atrophic changes covering the entire surface of the right buttock (Figure 1). The lesion was tender and warm with notable expression to light touch of purulent material through multiple fissures along the periphery. The patient reported no other symptoms, such as fever, chills, cough, or fatigue. On physical examination, vital signs were within normal limits, the skin demonstrated no other significant changes, and the patient had no notable lymphadenopathy. On history, the patient reported the skin lesion had progressively increased over the past four years. She had been previously diagnosed with psoriasis and was treated with multiple topical therapies, including salicylic acid and potent topical corticosteroids without any relief. Further, the patient reported having a similar lesion (which was on her neck) as a child that was surgically removed in Mexico. She had been Bacille Calmette-Guérin (BCG)-vaccinated in the past.
{kind=link}
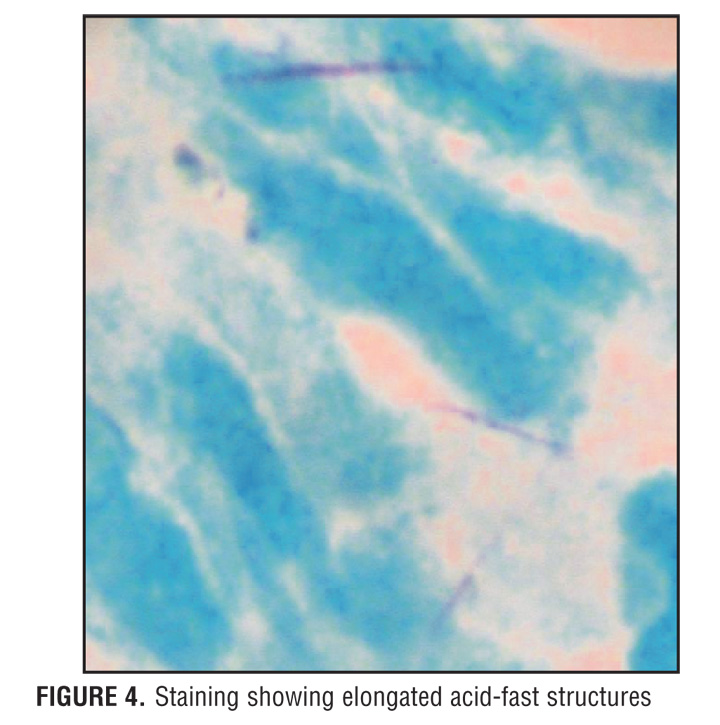
Serum QuantiFERON®-TB Gold (QFT-G; Cellestis Inc.,Valencia, California) testing was performed along with tissue cultures and skin biopsy with histological analysis. Histopathology of the plaque showed pseudoepitheliomatous hyperplasia and neutrophilic microabscesses in the epidermis. The dermis contained a mixed neutrophilic and granulomatous infiltrate (Figures 2 and 3). Acid-fast bacillus (AFB) staining showed rare elongated acid-fast structures suggestive of TB infection (Figure 4). Culture from lesional tissue grew Mycobacterium tuberculosis and serum QFT-G testing was positive. The patient was referred to infectious disease to rule out active TB infection. Sputum cultures were negative and a chest x-ray showed no active pulmonary disease.
{kind=link}
{kind=link}
A diagnosis of CTB was made based on the patient’s history, clinical picture, and diagnostic testing. Although an explicit classification of CTB could not be specified, lupus vulgaris (LV) and tuberculosis verrucosa cutis (TVC) are two variants of CTB that have been shown to occur in a previously sensitized individual, and her diagnosis was assumed to be one of these two variants. The patient was treated by infectious disease with multidrug TB therapy (pyrazinamide, rifampin, ethambutol, and isoniazid) resulting in lesion clearance at three months. Currently, the patient remains free of tuberculous disease.
Discussion
CTB describes dermatological manifestations of TB involving the skin, which can be caused by Mycobacterium tuberculosis, Mycobacterium bovis, and the BCG vaccination. These lesions can be acquired exogenously or endogenously, although the former is significantly less common. TB is one of the most common, rampant infectious diseases in underdeveloped countries, and the number of cases in industrialized countries has increased in recent years as a result of the increased incidence of HIV infection and increasing multidrug resistance.[6] Although CTB is reported as less than one percent of all cases of TB, it is important for practitioners to consider this infection when faced with a suggestive clinical picture.[7]
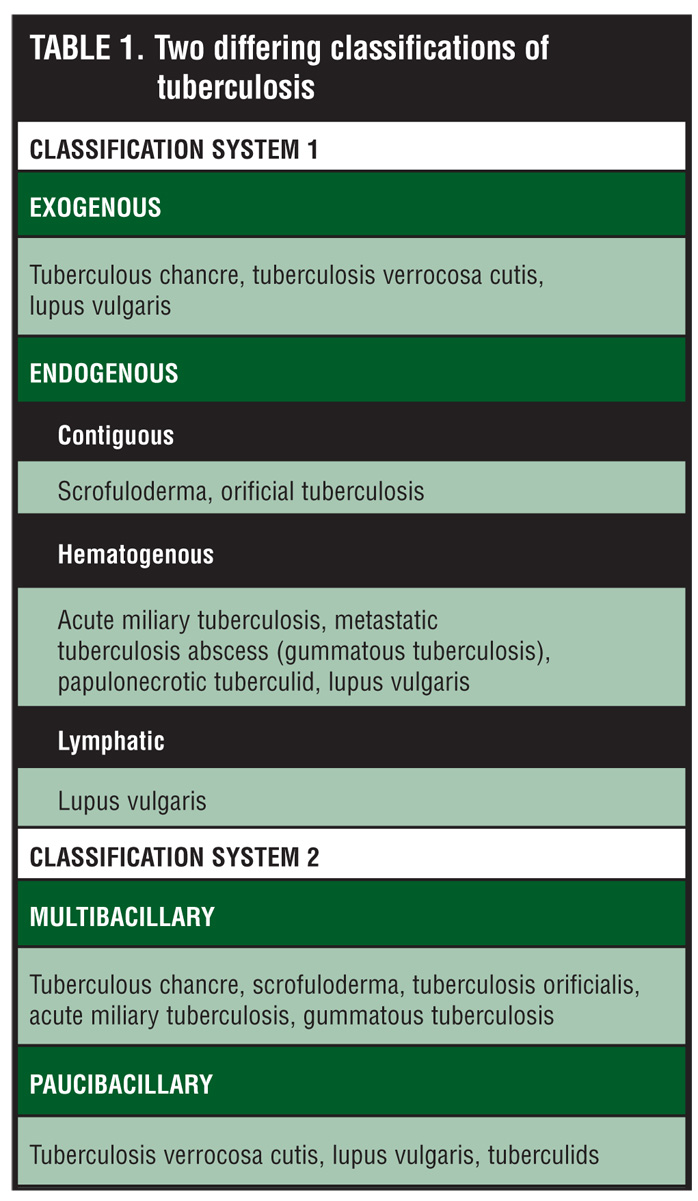
Early classification of CTB was based on lesion morphology. As knowledge of the disease increased, it became apparent that although lesions appeared clinically similar, their development, progression, and prognosis were different. Tappeiner and Wolff proposed the most widely accepted classification based on the route of infection (Table 1).[5,8] Exogenous inoculation occurs after the direct inoculation of Mycobacterium tuberculosis into the skin of a person who is susceptible to infection. This leads to TVC, tuberculosis chancre, and some cases of LV. Endogenous infection occurs in patients who were previously infected either by lymphatic spread, hematogenous spread, or contiguous extension. Lymphatic spread is seen occasionally in LV. Hematogenous spread is seen in acute miliary TB, metastatic TB abscess (gummatous TB), papulonecrotic tuberculid (PNT), and LV. Contiguous extension is seen in scrofuloderma and orificial tuberculosis.
{kind=link}
An additional classification system designed to enhance the Tappeiner and Wolff system included further distinction based on bacterial load. This system is extremely similar to Ridley and Jopling’s description of Mycobacterium leprae in Hanson’s disease. In the multibacillary forms, a plethora of mycobacteria can easily be identified on histological examination utilizing the Ziehl-Neelsen staining (AFB) method and culture. In the paucibacillary forms, sparse bacilli are seen on histological examination and culture isolation of mycobacteria is the exception rather than the rule.[1]
Multibacillary Forms
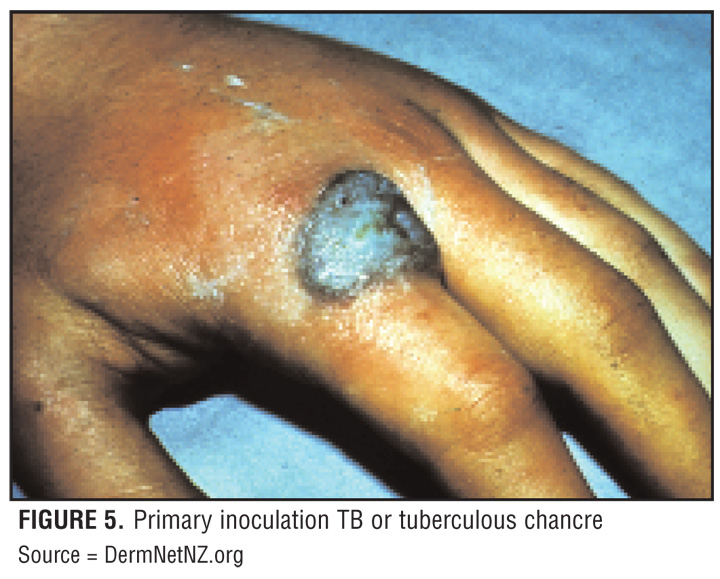
Primary inoculation TB (tuberculous chancre) typically follows a penetrating injury that results in the direct introduction of mycobacterium into the skin or mucosa of an individual with no previous TB infection. Within 2 to 4 weeks, an inflammatory papule develops at the inoculation site and evolves into a firm, shallow, non-tender, nonhealing, undermined ulcer with a granulomatous base (Figure 5).[3,5,9] Painless, regional lymphadenopathy is frequently apparent around the time a tuberculin skin test (TST) converts to positive.
{kind=link}
Scrofuloderma is the most common form of CTB in children and historically was seen after consumption of milk contaminated with Mycobacterium bovis. It results as a direct extension from an underlying TB focus, such as a regional lymph node or infected bone or joint, to the overlying skin. Lesions present as firm, painless, subcutaneous, red-brown nodules overlying an infected focus, which gradually enlarge and suppurate forming ulcers and sinus tracts that drain watery, purulent, or caseous material (Figure 6). Skin biopsy reveals tuberculoid granuloma surrounding areas of wedge-shaped necrosis. Culture, smear, or biopsy will demonstrate the organisms and confirm the diagnosis in a TST-positive individual.[9] The ulcers may heal spontaneously with scarring.
{kind=link}
TB cutis orificialis (TBCO) affects individuals with dramatically impaired cell-mediated immunity and advanced TB in other organs, such as the gastrointestinal tract and lungs. The oral, nasal, anal, and vulval regions become infected with Mycobacterium tuberculosis by autoinoculation from active infectious sites that are draining.[5] The red-yellow nodules break down and form painful, soft, circular or irregularly shaped “punched-out” ulcers with a pseudomembranous fibrinous base.[5,6] TST may or may not be positive, although organisms are easily seen on skin biopsy in the deep dermis and ulcer walls.[9] The presence of TBCO heralds a poor prognosis, as patients tend to have severe internal organ disease prior to skin manifestations.
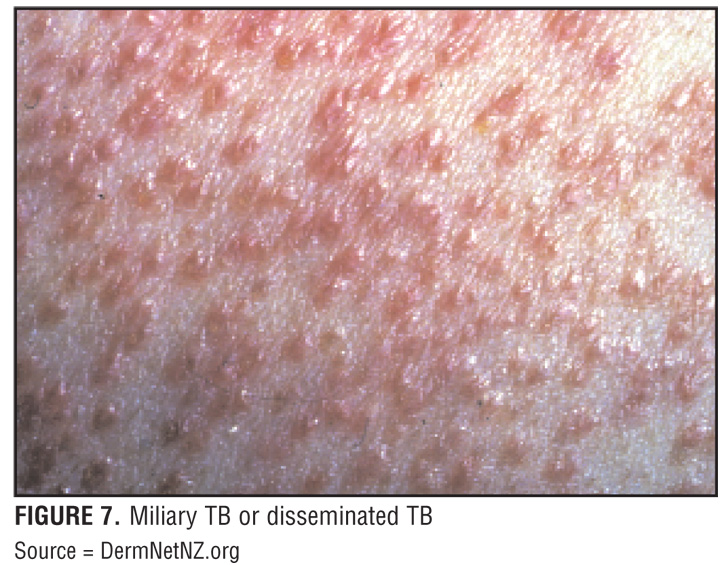
Miliary TB (disseminated TB) is characterized by a wide dissemination of Mycobacterium tuberculosis into the body and shows a distinctive pattern on chest x-ray of multiple, tiny lesions (millet-sized) distributed throughout the lung fields. Miliary TB may hematogenously infect any number of organs, including the lungs, liver, and spleen, in patients with advanced TB disease. There is a systemic failure of the cell-mediated immune system that allows and facilitates the spread of infection resulting in rapid deterioration and death.[3] Certain events, infections, and medications that suppress the body’s cell-mediated immune system can precipitate this infection. Although miliary TB has historically been extremely rare and well known for its occurrence in children, it is an increasingly serious infection in immunosuppressed patients, such as those infected with HIV, on long-term oral corticosteroid therapy, or on other immunosuppressive therapies for organ transplant or inflammatory or autoimmune conditions. Cutaneous skin lesions consist of small, erythematous to violaceous papules or pustules with hemorrhagic necrosis and umbilication affecting a substantial portion of the body (Figure 7). If healing occurs, lesions leave atrophic, depressed scars surrounded by a brownish, hyperpigmented halo. TST is typically negative because of anergy. Skin biopsy with histological examination reveals numerous microabscesses containing neutrophils and numerous mycobacterial organisms.[3] Confirmation of the diagnosis requires cultures of sputum, blood, and skin lesions, as well as diagnostic tests, such as bronchoscopy, chest x-ray, or computed tomography of the chest. Prognosis is poor, as affected individuals tend to be very ill at initial presentation (i.e., they have HIV, cancer, and/or are immunosuppressed).
{kind=link}
Metastatic TB abscesses (TB gumma) can arise from breakdown of an old healed tubercle that still contains live organisms or from cell-mediated immune defense inhibition that reactivates.[1,3] TB gumma is usually seen in malnourished children and immunosuppressed adults.[5] Single or multiple nontender, fluctuant nodules develop forming draining sinus abscesses unless surgically incised and drained. Nodules can occur at any location without any specific predominance. Histological examination reveals massive skin necrosis with copious mycobacterial organisms. TST is variable.
Paucibacillary Forms
TVC occurs after direct inoculation of TB into the skin of people who were previously infected. It manifests as a painless, solitary, purplish or brownish-red warty plaque that may extend peripherally causing central atrophy or form fissures that exude pus or keratinous material (Figure 8).[5,6] On physical examination, there is often lymphadenopathy. Skin biopsy with histological examination reveals pseudocarcinomatous hyperplasia with noncaseating tuberculous granulomata without mycobacteria seen or cultured. Skin lesions may evolve and persist for years, although spontaneous resolution can also occur. These lesions respond to typical anti-TB therapy of a combination of antibiotics given over months to years.
{kind=link}
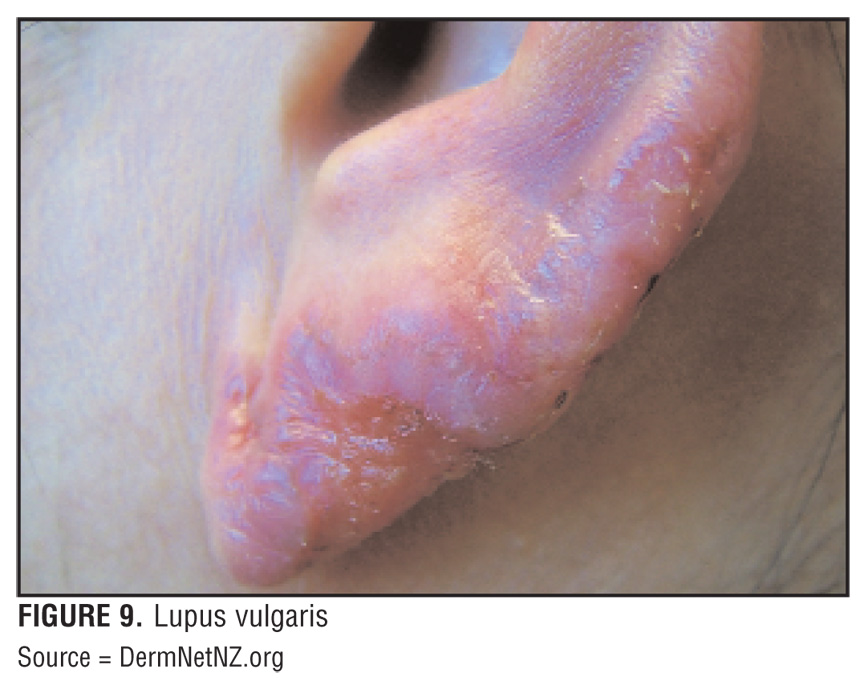
LV is a chronic and progressive form of CTB that is widely described as the most common form of CTB with a multitude of presentations. Lesions occur in normal skin as a result of direct extension from underlying deeper TB focus, by lymphatic or hematogenous spread, after primary inoculation, after BCG vaccination, or in scars of old scrofuloderma.[10] Lesions usually are small, solitary, nodular, sharply defined, reddish-brown lesions with a gelatinous consistency (called apple-jelly nodules) on the head and neck of individuals in Western countries while those individuals in tropical and subtropical areas present with lesions on the lower extremities or buttocks (Figure 9). Clinical variations exist and are defined as 1) classic plaque or keratotic; 2) hypertrophic; 3) ulcerative; and 4) vegetating. The plaque type begins as discrete, red-brown papules that coalesce and form plaques with a slightly elevated verrucas border and central atrophy. The consistency of the plaque is soft and gelatinous and has a classic apple-jelly appearance on dermoscopic examination. Persistent lesions may damage underlying tissue and ulcerate causing severe disfigurement and an increased risk of cancer formation. Skin biopsy with histological examination reveals tuberculous granulomas with few to no bacilli. Confirmation by culture is rare, even though an individual’s TST is usually positive.
{kind=link}
Tuberculids
The relationship between tuberculids and TB continues to be debated. Tuberculids are generalized exanthems in patients with a moderate or high degree of immunity to TB due to previous infection. Patients are usually in good health and show 1) positive TST; 2) tuberculous involvement (usually inactive) of viscera or lymph nodes; 3) negative staining and culture for pathogenic mycobacteria in affected tissue; and 4) skin lesions that heal with remission or treatment of TB. Classification includes three types: 1) PNT; 2) erythema induratum of Bazin (EIB); and 3) lichen scrofulosorum (LS). Tuberculids can be classified into two groups: true tuberculids and facultative tuberculids. The former classified because Mycobacterium tuberculosis plays a major etiologic role and the latter because Mycobacterium tuberculosis is one of several possibly etiologic agents. All were once believed to be a consequence of hypersensitivity to the presence of mycobacterial antigens within a host of previously acquired immunity to TB; however, most are now understood not to be uniquely caused by TB. PNT and LS are still widely accepted as true tuberculids and EIB as a facultative tuberculid. Whatever underlies the pathophysiology, a consensus has been reached that PNT and LS represent true hypersensitivity reactions rather than the result of a local CTB infection. This is based on the observation that these lesions have consistently failed to either stain positive for or culture mycobacterial organisms. Although the organisms are absent, mycobacterial DNA have been detected in biopsy specimens subjected to PCR. Furthermore, all tuberculids exhibit granulomatous inflammation and some degree of necrosis and vasculitis suggesting that these lesions are a result of released mycobacterial antigens in the setting of a concurrent or distant infection.
LS is an eruption of multiple, small, grouped, asymptomatic, firm, perifollicular, lichenoid papules or plaques most often affecting children or young adults that progresses and subsides within weeks to months without scarring.[3] Skin biopsy with histological analysis shows superficial, perifollicular, epithelioid granulomas surrounding hair follicles and sweat glands without evidence of necrosis. Typically no AFB are visualized histologically, although TST is often very remarkable.
EIB is a TB-associated panniculitis that presents with multiple, painful, recurring, ulcerated nodules that affect the lower limbs of women (Figure 10).[3,5] Pre-existing vascular disease may predispose patients to lesions during exposure to cold weather. Lesions are chronic; slow to resolve, if at all; and result in atrophic hyperpigmented scarring after several months. Histology should show three of four of the following elements: 1) septal panniculitis; 2) fat necrosis; 3) small or large vessel vasculitis; and 4) granulomas. Although patients show TB skin hypersensitivity, AFB are rarely identified. A 2005 study in Spain demonstrated that about 10 percent of cases were positive for Mycobacterium tuberculosis using PCR technique of identification.[11] In a case series and literature review, Bayer-Garner et al found that organisms, such as Mycobacterium bovis and Mycobacterium marinum, may also be involved as the etiology of EIB, although no identification was found during their investigation. They suggested that EIB has diverse etiologies with varying pathogeneses leading to similar histological changes, and the cases analyzed may not have had an infectious etiology (suggesting a facultative tuberculid picture).[12]
{kind=link}
Diagnosis
Diagnosis of CTB is complicated and requires a full work-up, including a detailed history and physical examination; careful consideration of clinical presentation; TST; serum QFT-G (and possibly other laboratory testing); skin biopsy with histological analysis and special staining methods for identification of AFB; and the use of other diagnostic tests, such as chest x-ray and sputum culture. The QFT-G is an in-vitro diagnostic aid that measures a component of cell-mediated immunity to Mycobacterium tuberculosis and is based on the quantification of interferon-gamma released from sensitized lymphocyte. QFT-G was approved in 2005 by the US Food and Drug Administration for the diagnosis of both latent and active TB infections. The antigens used in QFT-G are not shared by BCG vaccine strain or by nontuberculous mycobacterium. According to the Centers for Disease Control and Prevention guidelines of 2005, QFT-G can be used in place of the TST as it has increased specificity, lack of cross-reactivity to BCG, and convenience for both patient and provider.[13] Concordance rates between TST and QFT-G range from 60 to 90 percent. The cost effectiveness of QFT-G test still needs to be studied.[14]
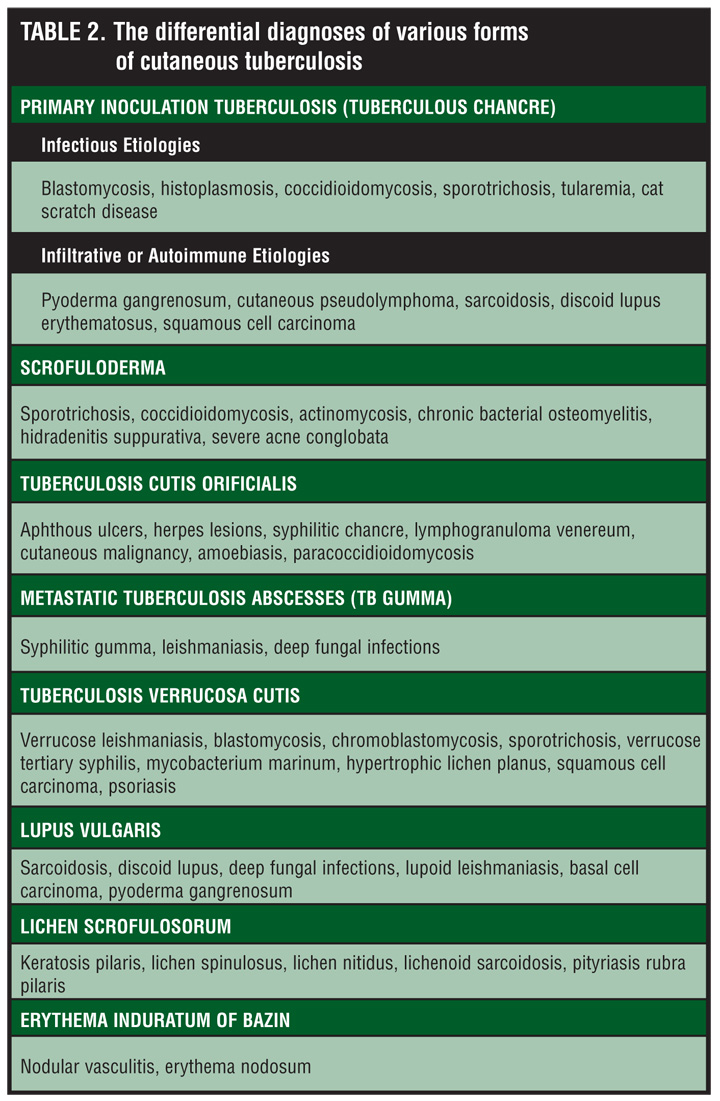
Mycobacterial culture remains the most reliable method to determine the presence of mycobacteria and their sensitivities, but the yield is often low and often takes many weeks.[2,9,16] Culture sensitivity is much lower than specificity, with sources ranging from 80 to 85 percent and 98.5 percent, respectively.[15,16] Mycobacterial growth is better on an egg-based medium, but quicker on agar medium. Liquid systems allow for rapid growth (1–3 weeks), while growth on solid media can take from 3 to 8 weeks. Two cases of EIB have been confirmed using guinea pig inoculation.[17] An AFB smear is useful if lesions have a high bacterial load as seen in LS, miliary TB, and TB gumma. With the advent of polymerase chain reaction (PCR), even the smallest tissue sample can be analyzed and amplified for mycobacterial DNA sequences, confirming its presence. In the future, it is believed that PCR will become more advanced to detect Mycobacterium tuberculosis in all lesions. Currently, PCR appears to be the most useful in multibacillary forms of CTB.[18,19] In one report of AFB-negative specimens, the overall sensitivity of PCR was found to be 50 to 72 percent.20 Another source reported AFB-positive respiratory specimens to have a sensitivity and specificity of 95 and 98 percent, respectively.15 In a comparison study of PCR and standard culture technique in pulmonary TB, one group found the positive rate of PCR was 82 percent compared to 16 percent in standard culture.[21] Margall et al detected Mycobacterium tuberculosis DNA in 77 percent of cases of various types of CTB.[4] Although PCR has shown to have high specificity and good positive predictive value, it seems to work best as a confirmatory test in patients with a high pre-test probability.[22] In multibacillary CTB, PCR has the highest likelihood of yield. Nonetheless, a combination of diagnostic tests is needed when a case of CTB is suspected to confirm a diagnosis. In developing countries, PCR is not always readily available and therefore physicians must rely on a positive response to anti-TB drugs to confirm difficult cases.[18,20,23] It is essential to search for extracutaneous foci of TB by urine, blood, and sputum samples; x-ray or CT scan of the chest; and bone scans. Often, there is a delay in the diagnosis because CTB is not always considered in the differential diagnosis of atypical or nonhealing skin lesions (Table 2). It is imperative that physicians have a high index of suspicion in high-risk patients and in atypical presentations.
{kind=link}
Treatment
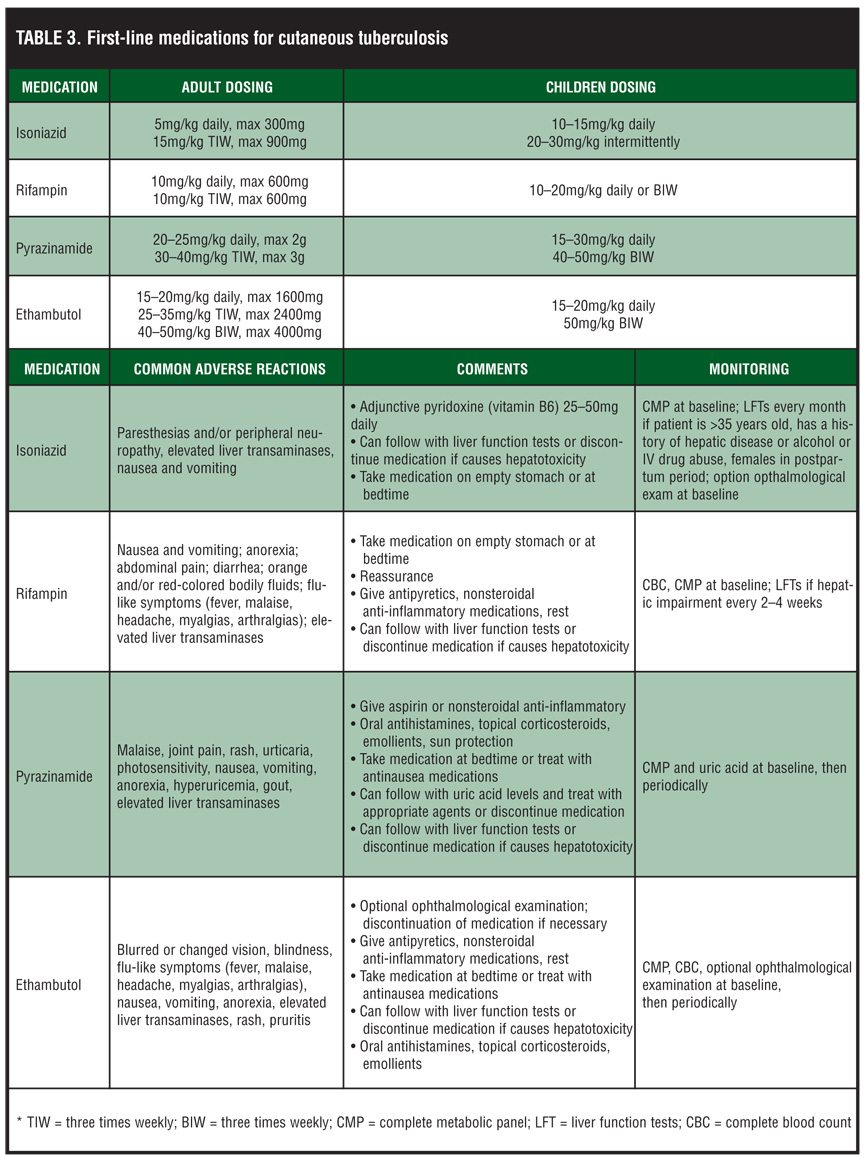
CTB treatment is the same as that for systemic TB and consists of long, multidrug therapy (Table 3). First, the chemotherapeutic treatment of TB is divided into two phases: 1) an intensive or bactericidal phase, designed to rapidly reduce the total body burden of Mycobacterium tuberculosis; and 2) a continuation or sterilizing phase. The most commonly used drugs are isoniazid, rifampin, pyrazinamide, and either ethambutol or streptomycin.[3,5,24] After eight weeks of therapy, the patients are considered no longer infectious, but still require longer term treatment for eradication. The continuation or sterilizing phase is designed to execute the remaining bacteria that resist the initial intensive or bactericidal phase. It is not clear why some of the bacteria resist the initial treatment, but the first-line drugs are typically highly effective. If the patient responded positively to isoniazid and rifampin, both are continued either daily or two or three times weekly for the second phase. Surgical intervention may be considered for the treatment of LV, TVC, and LS in recalcitrant cases.[5,6]
{kind=link}
Several considerations must be made prior to multidrug therapy in order to tailor the treatment to an individual patient. Considerations include 1) overall general health condition, including the immunity level of the patient; 2) the type of cutaneous involvement; 3) the stage of the disease; and 4) patient compliance with the duration of treatment and possible medication side effects. Adherence with treatment is especially important as improper use of anti-TB therapy can contribute to unwanted treatment side effects and the development of drug resistance that further facilities the spread of disease. Directly observed treatment involves observed therapy by personnel from the public health department to help increase patient adherence and control an infection that is a public health concern.
Conclusion
Tuberculosis is a serious infection that affects many people worldwide, with a recent increasing prevalence especially in high-risk patients, such as those from endemic countries, in an immunocompromised state, with a history of previous tuberculosis infection, and/or with multiple comorbidities. Although the incidence of CTB is rare, it should be considered in patients presenting with atypical skin lesions suggestive of an underlying infectious etiology. It is imperative that physicians have a high index of suspicion in order to quickly and effectively diagnose and treat these substantially morbid skin conditions. This case report demonstrates the importance of a proper history and physical examination as well as diligent laboratory and diagnostic testing in determining the etiology of a suspicious and treatment-resistant skin lesion. Prompt consideration leads to a swift diagnosis and proper treatment resulting in high patient satisfaction.
Acknowledgment
The authors would like to thank Brian Marciniak for his help in editing this paper.
References
1. Bravo FG, Gotuzzo E. Cutaneous tuberculosis. Clin Dermatol. 2007;25(2):173–180.
2. Fariña MC, Gegundez MI, Piqué E, et al. Cutaneous tuberculosis: a clinical, histopathologic, and bacteriologic study. J Am Acad Dermatol. 1995;33(3):433–440.
3. MacGregor RR. Cutaneous tuberculosis. Clin Dermatol. 1995;13(3):245–255.
4. Bhutto AM, Solangi A, Khaskhely NM, et al. Clinical and epidemiological observations of cutaneous tuberculosis in Larkana, Pakistan. Int J Dermatol. 2002;41(3):159–165.
5. Barbagallo J, Tager P, Ingleton R, et al. Cutaneous tuberculosis: diagnosis and treatment. Am J Clin Dermatol. 2002;3(5):319–328.
6. Handog EB, Gabriel TG, Pineda RT. Management of cutaneous tuberculosis. Dermatol Ther. 2008;21(3): 154–161.
7. Rai VM, Shenoi SD, Gowrinath. Tuberculous gluteal abscess coexisting with scrofuloderma and tubercular lymphadenitis. Dermatol Online J. 2005;11(3):14.
8. Lai-Chong JE, Perez A, Tang V, et al. Cutaneous manifestations of tuberculosis. Clin Exp Dermatol. 2007;32(4):461–466.
9. Brown FS, Anderson RH, Burnett JW. Cutaneous tuberculosis. J Am Acad Dermatol. 1982;6(1):101–106.
10. Marcoval J, Servitje O, Moreno A, et al. Lupus vulgaris. Clinical, histopathologic, and bacteriologic study of 10 cases. J Am Acad Dermatol. 1992;26(3 Pt 2):404–407.
11. Vieites B, Suárez-Peñaranda JM, Pérez Del Molino ML, et al. Recovery of Mycobacterium tuberculosis DNA in biopsies of erythema induratum—results in a series of patients using an improved polymerase chain reaction technique. Br J Dermatol. 2005;152(6):1394–1396.
12. Bayer-Garner IB, Cox MD, Scott MA, Smoller BR. Mycobacteria other than Mycobacterium tuberculosis are not present in erythema induratum/nodular vasculitis: a case series and literature review of the clinical and histologic findings. J Cutan Pathol. 2005;32(3):220–226.
13. National Tuberculosis Controllers Association; Centers for Disease Control and Prevention (CDC). Guidelines for the investigation of contacts of persons with infectious tuberculosis. Recommendations from the National Tuberculosis Controllers Association and CDC. MMWR Recomm Rep. 2005;54(RR-15):1–47.
14. Hernandez C, Cetner AS, Jordan JE, et al. Tuberculosis in the age of biologic therapy. J Am Acad Dermatol. 2008;59(3):363–380.
15. Diagnostic Standards and Classification of Tuberculosis in Adults and Children. This official statement of the American Thoracic Society and the Centers for Disease Control and Prevention was adopted by the ATS Board of Directors, July 1999. This statement was endorsed by the Council of the Infectious Disease Society of America, September 1999. Am J Respir Crit Care Med. 2000;161(4 Pt 1):1376–1395.
16. API Consensus Expert Committee. API TB Consensus Guidelines 2006: Management of pulmonary tuberculosis, extra-pulmonary tuberculosis and tuberculosis in special situations. J Assoc Physicians India. 2006;54:219–234.
17. Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin. A clinicopathological study of 20 cases and detection of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17(4):350–356.
18. Tan SH, Tan BH, Goh CL, et al. Detection of Mycobacterium tuberculosis DNA using polymerase chain reaction in cutaneous tuberculosis and tuberculids. Int J Dermatol. 1999;38(2):122–127.
19. Pai M. The accuracy and reliability of nucleic acid amplification tests in the diagnosis of tuberculosis. Natl Med J India. 2004;17(5):233–236.
20. Hsiao PF, Tzen CY, Chen HC, Su HY. Polymerase chain reaction based detection of Mycobacterium tuberculosis in tissues showing granulomatous inflammation without demonstrable acid-fast bacilli. Int J Dermatol. 2003;42(4): 281–286.
21. Sun YS, Wen JM, Lü WX, et al. Comparison study on polymerase chain reaction (PCR) and standard culture technique in detecting mycobacterium tuberculosis to diagnose of joint tuberculosis. Zhongguo Gu Shang. 2009;22(7):504–506.
22. Dinnes J, Deeks J, Kunst H, et al. A systematic review of rapid diagnostic tests for the detection of tuberculosis infection. Health Technol Assess. 2007;11(3):1–196.
23. Ramam M, Mittal R, Ramesh V. How soon does cutaneous tuberculosis respond to treatment? Implications for a therapeutic test of diagnosis. Int J Dermatol. 2005;44(2): 121–124.
24. Blomberg B, Fourie B. Fixed-dose combination drugs for tuberculosis: application in standardised treatment regimens. Drugs. 2003;63(6):535–553.