
James Landero, DO
Abilene, Texas
Abstract
The postural orthostatic tachycardia syndrome is a disease characterized by excessively increased heart rate during orthostatic challenge associated with symptoms of orthostatic intolerance including dizziness, exercise intolerance, headache, fatigue, memory problems, nausea, blurred vision, pallor, and sweating, which improve with recumbence. Postural orthostatic tachycardia syndrome patients may present with a multitude of additional symptoms that are attributable to vascular vasoconstriction. Observed signs and symptoms in a patient with postural orthostatic tachycardia syndrome include tachycardia at rest, exaggerated heart rate increase with upright position and exercise, crushing chest pain, tremor, syncope, loss of vision, confusion, migraines, fatigue, heat intolerance, parasthesia, dysesthesia, allodynia, altered traditional senses, and thermoregulatory abnormalities. There are a number of possible dermatological manifestations of postural orthostatic tachycardia syndrome easily explained by its recently discovered pathophysiology. The author reports the case of a 22-year-old woman with moderate-to-severe postural orthostatic tachycardia syndrome with numerous dermatological manifestations attributable to the disease process. The cutaneous manifestations observed in this patient are diverse and most noticeable during postural orthostatic tachycardia syndrome flares. The most distinct are evanescent, hyperemic, sharply demarcated, irregular patches on the chest and neck area that resolve upon diascopy. This distinct “evanescent hyperemia” disappears spontaneously after seconds to minutes and reappears unexpectedly. Other observed dermatological manifestations of this systemic disease include Raynaud’s phenomenon, koilonychia, onychodystrophy, madarosis, dysesthesia, allodynia, telogen effluvium, increased capillary refill time, and livedo reticularis. The treatment of this disease poses a great challenge. The author reports the unprecedented use of an oral angiotensin II type 1 receptor antagonist resulting in remarkable improvement. (J Clin Aesthet Dermatol. 2014;7(8):41–47.)
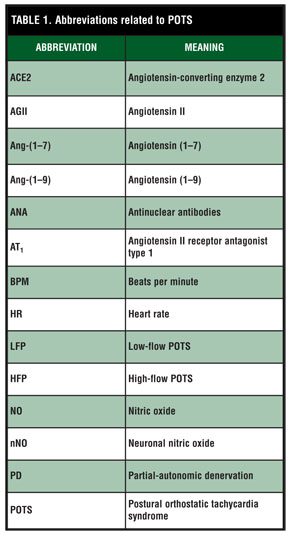
The postural orthostatic tachycardia syndrome (POTS, Table 1) is a relatively new disease with a multitude of systemic implications.[1] The author discusses systemic involvement and focuss on dermatological manifestations of POTS that are largely lacking in the literature. Until recent years, the pathogenesis of POTS has been largely unknown. Due to recent developments, targets have been exposed to guide treatment. The author reports the case of a patient with moderate-to-severe POTS with several systemic and dermatological manifestations as well as successful treatment with an angiotensin II type 1 receptor antagonist.
{kind=link}
Case report
A 22-year-old female patient described suffering from episodes of heat exhaustion, dizziness, presyncope, and exercise intolerance largely attributed to anxiety, heat stroke, low glucose, and self-induced phenomena beginning in childhood. Gradual progression of the disease resulted in episodes of syncope and palpitations. During her teenage years, she developed intermittent crushing chest pain, migraines, tremor, confusion, and a burning sensation of her skin. Frequent visits to the emergency department and hospitalizations forced her to take leave from college. Her past medical history is significant for attention deficit and hyperactivity disorder, atopic dermatitis, migraines, chronic anemia from presumed menometrorrhagia, and motor vehicle accidents resulting in head trauma requiring hospitalization and cutaneous repair. Medications include lisdexamfetamine (Vyvanse) 60mg daily, oral contraceptive, a multivitamin, and occasional acetaminophen use for migraines. She is allergic to penicillin and its derivatives and has multiple drug intolerances including hydrocodone, benadryl, and benzodiazepines. Patient denies alcohol, tobacco, illicit drugs, and supplements. Incidentally, she suffers from allergic contact dermatitis to urushiol and its associated cross-reactions. She developed angioedema shortly after consuming mango.
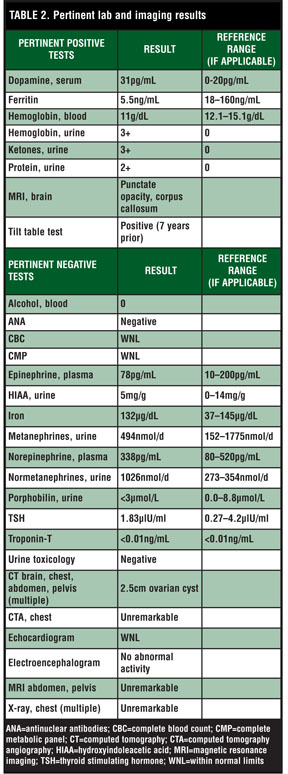
During a period of seven years, she was evaluated and frequently required hospital admissions during flares of her condition. She displayed persistent sinus tachycardia ranging from 100 to 200 beats per minute (bpm), confusion, chest pain, and vision changes among many other symptoms. She was typically treated with beta-blockers, anxiolytics, and volume expansion. Anxiolytics caused hallucinations during the early course of her medical history, at times contributing to the development of hypertensive crises requiring intensive care unit monitoring (Table 2).
During the author’s examination in the emergency department of one such flare, the patient displayed an evanescent, hyperemic, sharply demarcated patch over the chest and neck that resolved on diascopy. This evanescent hyperemia typically persists seconds to minutes before spontaneously disappearing and reappearing for the duration of the flare. There was also a network of macular, violaceous, connecting rings forming a netlike pattern on her distal and proximal extremities consistent with livedo reticularis. The patient has apparent acrocyanosis, koilonychia, >2 second capillary refill, a resting tremor affecting both hands, and patchy loss of eyelashes on both upper and lower eyelids bilaterally. Her heart rate rises from approximately 110 to 165bpm after minimal head or limb movement while remaining supine. She complains of severe chest pain and is temporarily relieved by sublingual nitroglycerin. After a few minutes, she loses consciousness and becomes unresponsive to pain (thumb pressure). In-patient psychiatric evaluation was recommended by neurology at that time.
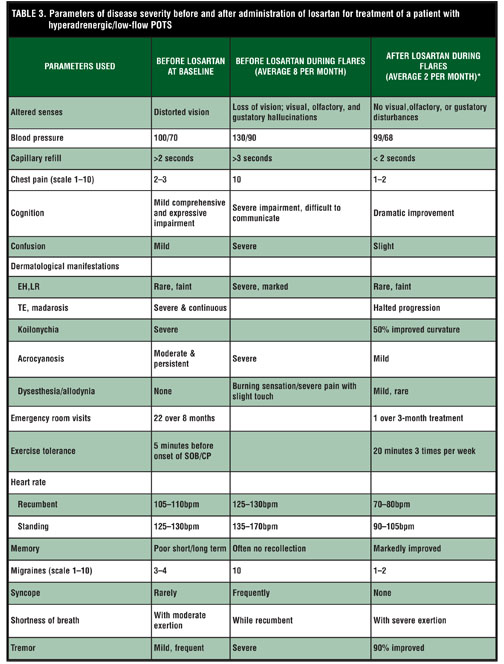
An article describing favorable local responses by Stewart[2] using intradermal losartan in patients with POTS established a possible treatment option for low-flow (and hyperadrenergic-type) POTS patients. The author’s patient discontinued all medications except for a multivitamin. Table 3 displays treatment results with the angiotensin II[1] antagonist losartan.
{kind=link}
{kind=link}
Discussion
Schondorf and Low[3] first described this poorly understood condition at the Mayo clinic’s department of neurology in 1993. POTS is defined as the presence of orthostatic intolerance associated with a heart rate (HR) increase of 30 beats per minute (bpm) or a rate that exceeds 120bpm within the first 10 minutes of standing or upright tilt, not associated with other chronic debilitating conditions (prolonged bed rest, medications that diminish vascular tone).[4] POTS patients typically have marked reduction in plasma volume[5] as well as stroke volume.[6] One of the key findings in POTS patients is the lack of orthostatic hypotension (fall of >20/10mmHg on standing), with most patients exhibiting a slight decline, no change, or even a modest increase in blood pressure.[4] The prevalence of POTS is estimated to be at least 500,000 patients in the United States alone and typically carries a female preponderance ratio of 5:1.[4]
Systemic manifestations
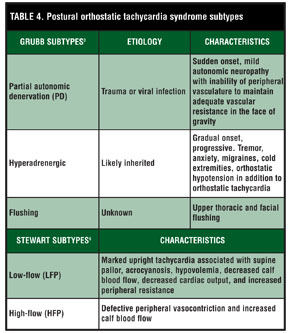
There are several subtypes of POTS. Grubb[4] describes three subtypes based on etiology and characteristics while Stewart[7] describes two subtypes based on clinical findings (Table 4). A typical “flare” of our patient’s condition is characterized by intermittent palpitations, shortness of breath, crushing chest pain that is responsive to nitroglycerin; tremor; syncope; dysesthesia; allodynia; blurry vision; loss of vision; seizure-like activity; insomnia; confusion; altered thought process; migraines; fatigue; exercise intolerance; heat intolerance; photophobia; altered taste, hearing, vision, touch and smell; and a considerably slow capillary refill >3 seconds. Minimal movement increases her heart rate by more than 30bpm and has a history of a positive tilt table test. She meets clinical criteria for both the low-flow and hyperadrenergic types of POTS. Flares are noticeably more frequent during menses.
{kind=link}
Pathogenesis
The diverse symptoms of POTS result from global inappropriate vasoconstriction and resultant impaired vascular hemodynamics. Peripheral arterial resistance is significantly increased and compensatory hyperemic blood flow is curtailed in POTS patients.[7] These observations are likely mediated by a blunted ACE2 pathway which results in increased serum levels of AGII, decreased Ang-(1-7), and resultant scant nitrous oxide (NO).[1,8] Increased serum norepinephrine levels3 may play a role. A mutation in the NE transporter SLC6A2 named A457P was recently implicated in the POTS phenotype.[9,10] The resting heart rate is considerably higher in POTS patients, while the muscle sympathetic nerve activity is much lower. POTS patients compound the deficit by experiencing exaggerated HR increase during tilt or change to upright position, while maintaining similar blood pressure to healthy patients.[11] The net effect of inappropriate vasoconstriction and impaired vascular dynamics lead to reduced neurocognition[12] through raised cerebrovascular resistance and a paradoxical decrease in cerebral blood flow while in upright posture.[13] Other perturbing observations in POTS include reduced stroke volume,[6] excessive heart rate response to orthostasis with propensity for edema,[11,14] decreased skeletal muscle pump activity,[15] abnormal quantitative sudomodor activity and thermoregulation,[2] and a multitude of pathophysiological effects.
Some of the resultant abnormalities in POTS patients’ serum include reduced plasma volume with a paradoxically unchanged plasma renin activity and low aldosterone.[5] They also have been found to have a significant red blood cell volume deficit that could be related to irregularities in erythropoietin by the kidney.[5] The discovery of angiotensin-(1-7) by Ferrario[16] and the consequential discovery of the ACE2 pathway by Tipnis in 2000[17] paved the way for current research in the pathophysiology of POTS with resultant treatment alternatives of greater efficacy.
Dermatological features
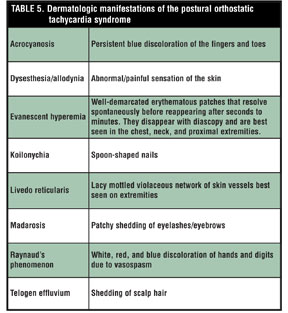
One can deduce from these findings that the dermatological findings of patients suffering from POTS can be attributed to the aforementioned pathophysiology. The most important etiological factors are the potent vasoconstriction and persistent hypoxia resulting from increased AG-II and decreased NO. The dermatological manifestations of the postural orthostatic tachycardia syndrome are listed in Table 5.
Koilonychia has been theorized to result from chronic iron deficiency. For instance, Ladakhi natives live at an altitude of 3,445 meters in India. The high altitudes cause inhabitants to develop koilonychia from increased erythropoiesis and depletion of iron stores. Thinning of the nail plate and koilonychia was found in 47 percent of 176 subjects studied.[18] Koilonychia has been found in a significant percentage of the population in the Himalayas and was thought to be due to retardation of nail plate growth from chronic hypoxia.[19]
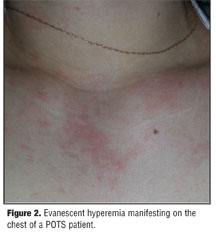
The two main causes of livedo reticularis are venodilation of vessels and deoxygenation of blood in the subpapillary venous plexus. Some of the underlying causes are altered autonomic nervous system function, circulating venodilators, and local hypoxia.[20] The tremor, Raynaud’s phenomenon, and dysesthesias observed in this patient are likely the result of persistent hypoxia, most pronounced in the distal extremities. The most characteristic dermatological sign of POTS is an “evanescent hyperemia.” In the author’s opinion, it is the result of local, uneven hyper-reactivity of the cutaneous vasculature to the potent constrictive effects of AGII. This lesion peculiarly disappears and reappears spontaneously in seconds to minutes during flares. This phenomenon may be highly characteristic or even pathognomonic if present in other hyperadrenergic/low-flow POTS patients. This cutaneous phenomenon is pictured in Figure 1
and Figure 2.
{kind=link}
{kind=link}
{kind=link}
Treatment
Current treatment options for POTS include a multitude of marginally effective medicinal modalities and behavioral techniques. One must be able to recognize the subtype of POTS and individualize treatment. Some general treatment options should encompass discontinuation of a drug that could be contributing to the patient’s symptoms[4] when possible. All patients should begin a gradual program of physical reconditioning. Fluid intake of approximately two liters per day and 3 to 5g of salt should be encouraged.[4] Elastic compression stockings may be helpful.[4] Medications that may be used to stabilize both the PD and hyperadrenergic forms include beta blockers,[21] stimulants,[22] selective serotonin re-uptake inhibitors/norepinephrine reuptake inhibitors (SSRI/NRI), pyridostigmine, fludrocortisones, midodrine (especially in PD), erythropoietin, octreotide, and clonidine (for hyperadrenergic form).[4]
The recent discovery of ACE2 in 2000 by Tipnis[17] and studies by Stewart implicating AGII, ang-(1-7)[1] and neuronal nitric oxide (nNO)[8] in the pathophysiology of POTS have unveiled potential novel application options in the management of this difficult disease. ATII[1] receptor antagonists, such as losartan, are one such option.
In contrary to popular belief, there have been studies proving that the excessive heart rate seen in POTS patients is not caused by anxiety, but is a physiological response that maintains arterial pressure during venous pooling.[23] Being that the author’s patient was not administered anxiolytics for the duration of treatment and her heart rate was significantly decreased, those results are consistent with his findings.
Conclusion
The postural orthostatic tachycardia syndrome is a fairly common, poorly known and understood, debilitating disease similar in functional impairment to that seen in congestive heart failure and chronic obstructive pulmonary disease.[4] POTS patients are commonly misdiagnosed as having panic disorder or severe anxiety.[4] The skin offers a “window” into the underlying pathology of the human body. As dermatologists, we have a clear advantage of recognizing POTS patients on the basis of cutaneous findings. These include livedo reticularis, koilonychia, acrocyanosis, telogen effluvium, madarosis, vascular cutaneous abnormalities, parasthesias, increased capillary refill, and other symptoms that are reasonably attributable to local abnormal vascular responses to AGII and an abnormal ACE2 pathway. Novel monotherapy with the AT1 receptor antagonist losartan was successful in this case and is a promising option for POTS, especially in the hyperadrenergic and low-flow subtypes. Longer clinical studies with a large patient population are needed prior to the widespread use of this modality. Nitrates may offer synergistic effects in difficult cases. Clinicians have an opportunity to recognize POTS patients and contribute to the improvement of those afflicted with this multi-organ disease by providing or simply guiding proper treatment.
References
1. Stewart JM, Ocon AJ, Clarke D, et al. Renin-angiotensin aldosterone system defects in cutaneous angiotensin-converting enzyme 2 and angiotensin-(1-7) production in postural tachycardia syndrome. Hypertension. 2009;53:767–774.
2. Stewart JM, Ocon AJ, Clarke D, et al. Defects in cutaneous antiotensin-converting enzyme 2 and antiotensin-(1-7) production in postural tachycardia syndrome. Hypertension. 2009;53(5):767–774.
3. Scondorf F, Low PA. Idiopathic postural orthostatic tachycardia syndrome. An attenuated form of acute pandysautonomia? Neurology. 1993;43(1):132–137.
4. Grubb B. Postural tachycardia syndrome. Circulation. 2008;117: 2814–2817.
5. Satish RR, Bioaggioni I, Yamhure PC, et al. Renin-aldosterone paradox and perturbed blood volume regulation underlying postural tachycardia syndrome. Circulation. 2005; 111:1574–1582.
6. Masuki S, Eisenach JH, Scharage WG, et al. Reduced stroke volume during exercise in postural tachycardia syndrome. J Appl Physiol. 2007;103(4):1128–1135.
7. Stewart JM, Medow MS, Montgomery LD. Local vascular responses affecting blood flow in postural tachycardia syndrome. Am J Physiol Heart Circ Physiol. 2003;285(6):H2749–H2756.
8. Stewart JM, Medow MS, Minson CT, Taneja I. Cutaneous neuronal nitric oxide is specifically decreased in postural tachycardia syndrome Am J Physiol Heart Circ Physiol. 2007;293(4):H2161–H2167.
9. Shirey-Rice JK, Klar R, Fentress HM, et al. Norepinephrine transporter A457P knock-in mice display key features of human postural orthostatic tachycardia syndrome. Dis Model Mech. 2013 April 4 [Epub ahead of print].
10. Hahn MK, Robertson D, Blakely RD. A mutation in the human norepinephrine transporter gene (SLC6A2) associated with orthostatic intolerance disrupts surface expression of mutant and wild-type transporters.J Neurosci. 2003;23(11):4470–4478.
11. Furlan R, Jacob G, Snell M, et al. Chronic orthostatic intolerance a disorder with discordant cardiac and vascular sympathetic control. Circulation. 1998;98:2154–2159.
12. Stewart JM, Medow MS, Messer ZR, et al. Postural neurocognitive and neuronal activated cerebral blood flow deficits in young chronic fatigue syndrome patients with postural tachycardia syndrome. Am J Physiol Heart Circ Physiol. 2012;302(5):H1185–H1194.
13. Jordan J, Shannon JR, Black BK, et al. Raised cerebrovascular resistance in idiopathic orthostatic intolerance evidence for sympathetic vasoconstriction. Hypertension. 1998;32:699–704.
14. Stewart JM, Weldon A. Vascular perturbations in the chronic orthostatic intolerance of the postural orthostatic tachycardia syndrome. J Appl Physiol. 2000;89(4):1505–1512.
15. Stewart JM, Medow MS, Montgomery LD, McLeod K. Decreased skeletal muscle pump activity in patients with postural tachycardia syndrome and low peripheral blood flow. Am J Physiol Heart Circ Physiol. 2004;286(3):H1216–H1222.
16. Ferrario CM. Angiotensin-converting enzyme 2 and angiotensin-(1-7) An evolving story in cardiovascular regulation. Hypertension. 2006;47:515–521.
17. Tipnis SR, Hooper NM, Hyde R, et al. A human homolog of angiotensin-converting enzyme. Cloning and functional expression as a captopril-insensitive carboxypeptidase. J Biol Chem. 2000;275(43):33238–33243.
18. Sawhney MP. Ladakhi koilonychia. Indian J Dermatol Venereol Leprol. 2003;69(2):79–80.
19. Patial RK. High altitude koilonychia. J Assoc Physicians India. 1999;47(4):406–408.
20. Gibbs MB, English JC, Zirwas MJ. Livedo reticularis: an update. J Am Acad Dermatol. 2005;52:1009–1019.
21. Arnold AC, Okamoto LE, Diedrich A, et al. Low-dose propranolol and exercise capacity in postural tachycardia syndrome: a randomized study. Neurology. 2013 April 24 [Epub ahead of print].
22. Kanjwal K, Saeed B, Karabin B, et al. Use of methylphenidate in the treatment of patients suffering from refractory postural tachycardia syndrome. Am J Ther. 2012;19(1):2–6.
23. Shizue Masuki, Eisenach JH, Johnson CP, et al. Excessive heart rate response to orthostatic stress in postural tachycardia syndrome is not caused by anxiety. J Appl Physiol. 2007;102(3):896–903.