
Lauren Geller, MD; Jamie Rosen, BA; Amylynne Frankel, MD; Gary Goldenberg, MD
Icahn School of Medicine at Mount Sinai, Department of Dermatology, New York, New York;
Icahn School of Medicine at Mount Sinai, New York, New York
Abstract
Background: Acne is typically regarded as an adolescent disease. A significant body of literature suggests a post-adolescent or adult form of acne. Female patients are known to experience perimenstrual acne flares, the exact prevalence of which is unknown. Objective: To establish a pattern of perimenstrual acne flare in adult women in order to better characterize the disorder. Methods: Subjects aged 18 and over were recruited during previously scheduled visits with their dermatologist at Mount Sinai Hospital in New York. An anonymous survey was distributed to women who reported their first menses at least six months earlier and had a complaint of acne within the last 30 days. Women <18 years of age and postmenopausal women were excluded from the study population. Results: Participants included women 18- to 29-years old (67%) and women 30- to 49-years old (33%). The ethnicity of respondents was Caucasian (50%), African American (20%), Latino (19%), Asian (5%), and Other (6%). The majority of participants with perimenstrual acne reported the onset of acne between the ages of 12 and 18 years. Sixty-five percent of participants reported that their acne symptoms were worse with their menses. Of those who reported perimenstrual acne symptoms, 56 percent reported worsening symptoms in the week preceding their menses, 17 percent reported worsening symptoms during their menses, three percent reported worsening symptoms after their menses, and 24 percent reported worsening symptoms throughout their cycle. Thirty-five percent of patients with perimenstrual acne reported oral contraceptive pill use. Conclusion: A significant number of adult women have perimenstrual acne symptoms. This study has proven to be useful in characterizing perimenstrual acne flare and is one of the first qualitative documentations of the presence and degree of this disorder. (J Clin Aesthet Dermatol. 2014;7(8):30–34.)
Acne is a chronic skin disease characterized by comedones, pustules, and papules and affects more than 85 percent of adolescents at some point in their lifetime.[1] Although acne has traditionally been thought of as a disorder of adolescence, a significant body of literature suggests a postadolescent or adult form of the disease.[2] Acne frequently continues into adulthood, the mean age of presentation for treatment being 24 years of age with 10 percent of visits occurring between the ages of 35 and 44 years.[1] Recent studies have reported that 50 percent of female patients with acne are over the age of 20.[3–5] The prevalence varies between sexes and age groups; studies report that adolescent acne predominantly affects males while postadolescent acne has a female predominance.[6]
There is a common medical and lay belief that women experience perimenstrual acne flares. However, the exact prevalence of premenstrual acne is unknown. Stoll et al7 found that there is an overall premenstrual flare rate of 44 percent, while Lucky et al8 found that 63 percent of women had an increase in the number of inflammatory acne lesions in the late luteal phase of the menstrual cycle.[7,8]
The pathophysiology of acne is largely influenced by hormonal regulation. Androgens, such as dihydrotestosterone (DHT) and dehydroepiandrosterone sulfate (DHEA-S), stimulate androgen receptors found in sebaceous glands and the outer root sheath of hair follicles. This results in the accumulation of sebum and keratin in follicles resulting in open and closed comedones and providing a growth medium for Propionibacterium acnes.[10] In the prepubertal period, a normal rise in serum androgens and an increased sensitivity of sebaceous glands to circulating androgens may contribute to the development of acne. Thus, hormonal therapy including spironolactone, an androgen receptor inhibitor, as well as oral contraceptive pills (OCPs), which inhibit androgen production by the ovaries, are frequently cited therapies to control acne in women.[11]
While premenstrual acne flare is a commonly reported phenomenon, there is little documentation of its true prevalence in adult women. This study aims to establish a pattern of perimenstrual acne flare in women of child-bearing potential in order to better characterize the disorder.
Methods
Study participants. Participants, age 18 and older, were recruited from an outpatient dermatology practice at Mount Sinai Hospital, which serves a diverse patient population. Subjects were recruited during previously scheduled visits with their dermatologist. Anonymous surveys were distributed to women who reported their first menses at least six months earlier and had a complaint of acne within the last 30 days. Female subjects under the age of 18 and postmenopausal women were excluded from the study. The Mount Sinai Institutional Review Board approved this study.
Subject questionnaire. An anonymous survey was developed by the authors based on previous literature as well as the experience of participating dermatologists. The survey consisted of 15 multiple choice and open-ended queries to identify patient demographic information as well as qualify their acne severity and prior treatment regimens. The survey was administered to 105 patients recruited from one dermatology practice.
Statistical analysis. Statistical analysis was performed using unpaired t-tests. Data was analyzed with Microsoft Excel 2012. A value of P<0.05 was considered significant.
Results
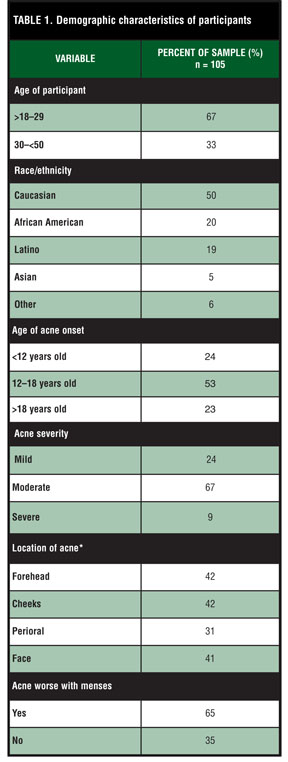
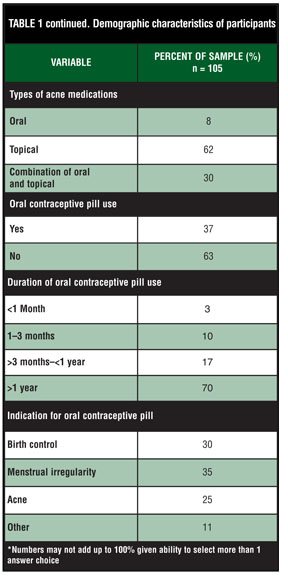
Demographics (Table 1 and Table 1 continued). The anonymous survey was completed by 105 participants. Women between the ages of 18 and 50 participated in the study: 18- to 29-years old (67%) and 30- to 50-years old (33%). Of those in the 18- to 29-year old group, 68 percent reported perimenstrual acne flares compared to 42 percent in the 30- to 50-year old group. Race and ethnicity were: Caucasian (50%), African-American (20%), Latino (19%), Asian (5%), and Other (6%). Within those groups, those who reported perimenstrual acne symptoms included: Caucasians (69%), African-Americans (61%), Latino (58%), Asian (60%) and other (50%).
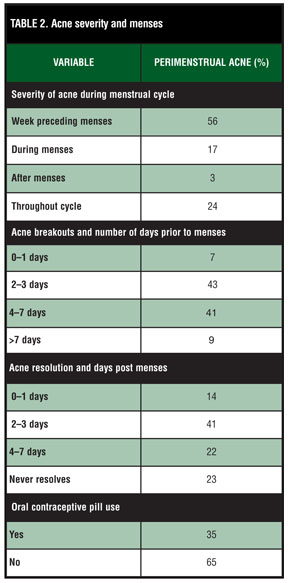
Acne severity and menses (Table 2). Sixty-five percent of participants reported that their acne symptoms were worse with their menses. Respondents graded the severity of their acne as mild (24%), moderate (67%), and severe (9%). The majority (53%) of participants reported the onset of acne between the ages of 12 and 18 years. Surveys revealed an equal distribution of acne around the face: forehead (42%), checks (42%), perioral (31%), and entire face (41%). There was no significant difference in the distribution of acne in those with premenstrual acne flare.
Of those who reported perimenstrual acne symptoms, 56 percent reported worsening symptoms in the week preceding their menses, 17 percent reported worsening symptoms during their menses, three percent reported worsening symptoms after their menses, and 24 percent reported worsening symptoms throughout their cycle. Of those with perimenstrual acne, 91 percent of participants noted that their acne breakouts began within the seven days prior to the onset of their menses and 77 percent noted that their acne disappeared within one week of its completion.
Women used a variety of topical (62%), oral (8%), and a combination of topical and oral medications (30%). Of the entire sample, 31 patients (37%) were using a hormonal contraceptive for a period of <1 month (3%), 1 to 3 months (10%), >3 months to <1 year (17%), and >1 year (70%). The indication for prescribing the OCP in perimenstrual acne patients included: birth control (30%), menstrual irregularity (35%), acne (25%), and other (11%). Thirty-five percent of patients with perimenstrual acne reported OCP use. Fifty-seven percent of patients with perimenstrual acne reported that they would be very likely to use a safe and effective topical treatment for perimenstrual acne symptoms.
{kind=link}
{kind=link}
{kind=link}
Discussion
The present study supports the notion that women experience acne exacerbation prior to the onset of their menses, with 65 percent of participants reporting perimenstrual acne flare. Prior to this study, little documentation existed about the pattern and prevalence of perimenstrual acne flare in adults. A recent review of the clinical and epidemiological literature on adult acne found that the prevalence of adult acne ranged from 41 to 51 percent.[12] One study documented menstrual periods as the most aggravating factor for acne flare in 78 percent of participants.[13] In 2001, Stoll et al7 studied the effect of the menstrual cycle on acne, revealing that among 400 participants, 44 percent of respondents experienced perimenstrual acne flare. Furthermore, Lucky8 quantitatively documented the presence and degree of flare by surveying acne lesion counts in the follicular and luteal phases of the menstrual cycle. The study revealed that 63 percent of adult women had more acne lesions in the late luteal phase of the menstrual cycle, with 23.2 percent of participants showing an increased number of total acne lesions, 25.3 percent being inflammatory lesions and 21.2 percent comedonal lesions.
While the relationship between acne and the menstrual cycle has been clearly described, the exact mechanism and causal association remains unknown.[9] Acne in the postadolescent patient is most frequently due to the persistence of adolescent acne, characterized by follicular hyperkeratinization, inflammation, colonization by P. acnes, and increased sebum production. However, postadolescent acne or late-onset adult acne remains differentiated from adolescent acne in that it presents as deep-seated, mild-to-moderate inflammatory, papulo-pustular lesions located on the lower third of the face, jawline, and neck.[14] The pathophysiology of postadolescent acne and underlying hormonal dysregulation in patients has been extensively investigated; however, the data remains controversial. Levels of testosterone, DHEA, and DHEA-S have been reported in some studies as elevated, and in others within normal range.[15,16] However, some studies have revealed that higher levels of free androgens and DHEA-S and lower levels of sex hormone binding globulin (SHBG) are strongly associated with adult onset acne in comparison to controls. Interestingly, these levels do not correlate with acne severity.17,18 Additionally, excess levels of androgens in the skin and sebaceous gland may promote sebum production and thus significantly impact the prevalence of acne in the postadolescent female.[19]
The incidence of perimenstrual acne flare among the postadolescent population suggests a need for therapies that target this cohort of women. Since a portion of postadolescent acne is simply a continuation of adolescent acne, many reports have suggested treating both populations in the same way. A review of recent literature found that sebum excretion is decreased perimenstrually, which may help to explain the effects of isotretinoin, an extremely successful treatment for severe acne that works by causing sebaceous gland atrophy.[20] Additionally, hormonal treatments may be a successful approach for treating perimenstrual acne flare in patients with elevated levels of androgens. The use of OCPs has improved acne severity in some women. A multicenter, randomized, double-blind, placebo-controlled trial evaluated the effect of norgestimate-ethinyl estradiol in the treatment of acne vulgaris, finding that the oral contraceptive group had a significant reduction in inflammatory lesions and total lesions compared to controls. Lower mean baseline levels of sex hormone binding globulin were found in the treatment arm, which decreases the availability and concentration of diffusible androgen for acne pathogenesis. The ethinyl estradiol component inhibits the production of ovarian androgens by inhibiting the secretion of pituitary gonadotropins. Antiandrogen therapies may be useful in the treatment of acne resistant to or rapidly relapsing after treatment with isotretinoin.[21] However, women obtaining contraception for acne treatment should avoid regimens containing androgenic progestins (i.e., norgestrel and levonorgestrel), as they can increase the level of free testosterone and thus complicate and exacerbate acne. Multiple studies have proven the efficacy of using oral contraceptives in the treatment of acne.[22–24] To our knowledge, there is no study that looks directly at the effects of OCPs on perimenstrual acne flare. However, given the hormonal nature of the menstrual cycle, use of OCPs may prove to be a successful therapeutic approach.
This study has several limitations. The questionnaire was only offered in English and thus only those able to communicate in English were recruited for the study. The study population was recruited from a single geographic area and included only persons attending the dermatology clinic, which may represent a cohort of individuals with more severe acne. Thus, further studies must confirm the prevalence and pattern of perimenstrual acne.
Furthermore, the study population comprised primarily young, postadolescent Caucasian women, which may not be entirely generalizable to other populations. In terms of technical weaknesses, because the questionnaires asked patients to report information after a significant time elapsed, self-reported symptoms and presentation is often subject to recall bias, which can be misleading and inaccurate.
The present study is one of the first to document the pattern and prevalence of perimenstrual acne among the postadolescent population. In this study, 65 percent of all participants reported worsening acne with their menses, the majority of whom reported worsening symptoms in the week preceding their menses. The authors’ findings for the prevalence of women with perimenstrual acne is comparable to the earlier studies by Lucky et al.[8] Conversely, the authors’ prevalence is slightly higher than the prevalence noted in Stoll et al,[7] which may reflect differences in study design and the smaller number of subjects in the study discussed herein. While this study has proven an association between acne exacerbations and a woman’s menstrual cycle, it also identified a significant gap in literature and lack of large-scale epidemiological studies that assess the incidence and clinical features that are involved in this disorder.
In conclusion, the results of this study highlight that perimenstrual acne flare is a significant and growing complaint affecting a large number of adult women. The study provides good evidence that acne is no longer simply a disorder of adolescence; postadolescent acne can be a devastating disorder with a significant impact on quality of life. The increasing prevalence of perimenstrual acne requires us to recognize this subset of women as an increasingly important population requiring treatment. For women with hormonal breakouts related to the menstrual cycle, hormonal therapy may be a helpful addition to the treatment armamentarium. However, given the dearth of literature and epidemiological studies, a large-scale cross-sectional analysis is needed to further evaluate the prevalence of perimenstural acne flare as well as improve clinical outcomes through the development of targeted therapeutics.
References
1. James WD. Acne. N Engl J Med. 2005;352:1463–1472.
2. Knaggs HE, Wood EJ, Rizer RL, et al. Post-adolescent acne. Int J Cosmet Sci. 2004;26(3):129–138.
3. Perkins AC, Maglione J, Hillebrand GG, et al. Acne vulgaris in women: prevalence across the life span. J Womens Health (Larchmt). 2012; 21(2): 223–230.
4. Khunger N, Kumar C. A clinic-epidemiological study of adult acne: is it different from adolescent acne? Indian J Dermatol Venereol Leprol. 2012;78(3):335–341.
5. Preneau S, Dreno B. Female Acne—a different subtype of teenager acne? J Eur Acad Dermatol Venereol. 2012;26(3):277–282.
6. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56.
7. Stoll S, Shalita AR, Webster GF, et al. The effect of the menstrual cycle on acne. J Am Acad Dermatol. 2001;45(6):957–960.
8. Lucky AW. Quantatitive documentation of a premenstrual flare of facial acne in adult women. Arch Dermatol. 2004;140:423–424.
9. Williams M, Cunliffe WJ. Explanation for premenstrual acne. Lancet. 1973;2(7837):1055–1057.
10. Thiboutot D. Acne: hormonal concepts and therapy. Clin Dermatol. 2004;22:419–428.
11. Katsambas A, Dessinioti C. Hormonal therapy for acne: why not as first line therapy? Facts and controversies. Clin Dermatol. 2010;28:17–23.
12. Preneau S, Dreno B. Female acne—a different subtype of teenager acne? J Eur Acad Dermatol Venereol. 2012;26:277–282.
13. Poli F, Dreno B, Verschoore M. An epidemiological study of acne in female adults: results of a survey conducted in France. J Eur Acad Dermatol Venereol. 2001;15:541–545.
14. Capitanio B, Sinagra JL, Bordignon V, et al. Underestimated clinical features of postadolescent acne. J Am Acad Dermatol. 2010;63(5):782–788.
15. Sultan C, Oliel V, Audran K, et al. Free and total plasma testosterone in men and women with acne. Acta Derm Venereol (Stockh). 1986;66:501–504.
16. Schiavone FH, Rietschel RL, Sgoulas D, et al. Elevated and free testosterone levels in women with acne. Arch Dermatol. 1983;119:799–802.
17. Seirafi H, Farnaghi F, Vasheghani-Farahani A, et al. Assessment of androgens in women with adult-onset acne. Int J Dermatol. 2007;46:1188–1191.
18. Darley CR, Kirby JD, Besser GM, et al. Circulating testosterone, sex hormone binding globulin and prolactin in women with late onset or persistent acne vulgaris. Br J Dermatol. 1982;106: 517–522.
19. Lookingbill DP, Horton R, Demers LM, et al. Tissue production of androgens in women with acne. J Am Acad Dermatol. 1985;12:481–487.
20 Knaggs HE, Wood EJ, Rizer RL, Mills OH. Post-adolescent acne. J Cosmet Sci. 2004;26:129–138.
21. Beylot C, Doutre MS, Beylot-Barry M. Oral contraceptives and cyproterone acetate in female acne treatment. J Dermatol. 1998; 196:148-152.
22. Lucky AW, Henderson TA, Olson WH, et al. Effectiveness of norgestimate and ethinyl estradiol in treating moderate acne vulgaris. J Am Acad Dermatol. 1997;37:746–754.
23. Olson WH, Lippman JS, Robisch DM. The duration of response to norgestimate and ethinyl oestradiol in the treatment of acne vulgaris. Int J Fertil Womens Med. 1998;43:286–289.
24. Ganceviciene R, Graziene V, Fimmel S, Zouboulis CC. Involvement of the corticotropin-releasing hormone system in the pathogenesis of acne vulgaris. Br J Dermatol. 2009;160:345–352.