
Yasemin Oram, MD; A. Deniz Akkaya, MD
Department of Dermatology, V.K. Foundation American Hospital of Istanbul,
Abstract
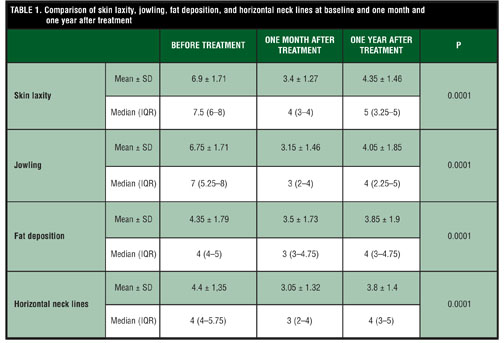
Objective: To assess the effectiveness of 10,600nm fractional CO2 laser for neck aging at one month and one year after treatment. Design/Setting/Participants/Measurement: Twenty patients underwent 10,600nm fractional CO2 laser treatment over the entire neck. Clinical features of the patients were classified according to Baker classification. The degrees of skin laxity, jowling, fat deposition, and horizontal neck lines were evaluated using a 9-point scale, prior to treatment at one month and one year after the treatment. The patients were independently assessed by the authors at two different times in a blinded fashion. Results: Skin laxity, jowling, fat deposition, and horizontal neck lines scores were significantly lower than the baseline values at one month and one year. One-year follow-up values of the same parameters were still significantly lower than the baseline. No persistent complication developed after treatment. Conclusion: The results of this study confirm that fractional CO2 neck rejuvenation is an effective treatment option with long-term efficacy for patients who mainly have skin laxity and jowling together with skin surface pigmentation. (J Clin Aesthet Dermatol. 2014;7(8):23–29.)
Aesthetic improvement of the aging neck remains one of the most challenging aspects of antiaging procedures. Although a variety of surgical and nonsurgical techniques have been targeted in this area, most of the patients become dissatisfied with the treatment results. This difficulty is mainly due to the complexity of the aging phenomenon of this particular area. The neck aging may be related to loss of skin quality, deposition of submental fat, decrease in muscle tone, changes in weight, and sun damage.[1]
Several methods have been recommended for the treatment of neck aging. These include tumescent liposuction, laser-assisted liposuction, minimally invasive skin tightening, radiofrequency, intense focused ultrasound, onabotulinum toxin A injections, ablative or nonablative laser resurfacing, and other surgical lifting procedures, either alone or in combination. A thorough understanding of the various components of neck aging is essential to select the appropriate therapy or combination therapies. Most of the patients require a combination of these treatment modalities to have a better clinical outcome as they exhibit several factors contributing to neck aging.[1–5]
In recent years, the concept of fractional photothermolysis has become very popular in skin rejuvenation by decreasing recovery time, risk of side effects, and complications while achieving clinical results approaching those seen with traditional CO2 laser resurfacing. Fractional CO2 laser produces an array of microthermal treatment zones in a pixelated fashion, with a confluent pattern of ablation and coagulation extending from the stratum corneum through the dermis. Rapid wound healing is provided by viable keratinocytes in the untreated islands of surrounding skin. Fractional CO2 laser has been shown to provide a safe and effective rejuvenation with significant effects on skin tightening and texture.[6,7]
Materials and methods
From January to April 2010, 20 female patients had fractional CO2 laser treatment for neck rejuvenation. Fitzpatrick skin types were II to IV. High quality standardized color photographs using a D70 Nikon digital camera were obtained. The patients provided informed consent forms and were independently assessed by the authors at two different times in a blinded fashion. The principles of the 1975 Declaration of Helsinki were followed.
Clinical features of the patients were classified according to Baker classification.[8] Type I patients have slight cervical skin laxity with submental fat and early jowls; Type II patients have moderate cervical skin laxity, moderate jowls and submental fat; Type III patients have moderate cervical skin laxity, but with significant jowling and active platysmal banding; Type IV patients have loose redundant cervical skin and folds below the cricoid, significant jowls, and active platysmal bands. The degrees of skin laxity (SL), jowling (J), fat deposition (FD), and horizontal neck lines (HNL) were evaluated using a 9-point scale (0=none, 1–3=mild, 4–6=moderate, and 7–9=severe) prior to treatment, after one month of treatment, and after one year of treatment.
The 10,600nm fractional CO2 laser (Candela QuadraLase, Candela, Wayland, Massachusetts) was used with laser parameters as 300-micron hand-piece attachment, 12–14W energy, 3.5msec pulse width, and 20- to 30-percent coverage (approximately 200–250 micron depth). Anesthetic cream (EMLA®, eutectic mixture of 2.5% lidocaine and 2.5% prilocaine) was applied under occlusion for one hour before the laser treatment. After cleaning the skin, the patients underwent a single pass laser treatment over the entire neck, avoiding overlap. Patients were instructed to use the prescribed antibiotic cream and moisturizer and to avoid sun exposure. They returned for follow-up visits at 3, 7, 14, 30, 90 days, and one year after treatment for the evaluation of clinical results and adverse effects. The effectiveness of the treatment was assessed clinically at one month and one year follow-up visits with the same scale system utilized at the baseline.
NCSS (Number Cruncher Statistical System) 2007 Statistical Software (Utah, USA) program for Windows was used for statistical calculations. The intraclass correlation coefficient (ICC) was calculated for the inter- and intraobserver reliability. Descriptive statistics were calculated, such as mean, standard deviation, median, and interquartile range. Friedman test was used to determine the differences in repeated measurements, Kruskal-Wallis test was used in the comparison of groups, and post hoc Dunn’s multiple comparison test was utilized in the comparison of subgroups. Statistical significance level was established as p<0.05.
Results
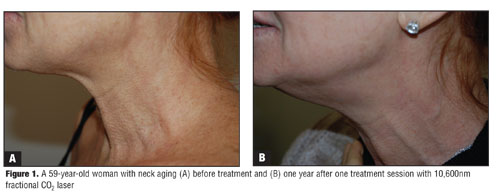
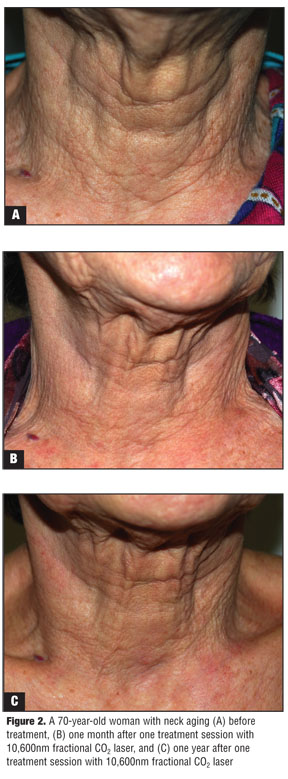
Overall, the patients tolerated the procedure and post-laser recovery period well. Patients ranged in age from 52 to 76 years with a mean age of 64.9 years. All patients developed a better skin texture and color at the end of one month and one year. For SL, J, FD, and HNL, ICCs for inter- and intraobserver reliability ranged between 0.879 and 0.912 and 0.964 and 0.978, respectively, indicating a strong agreement. SL, J, FD, and HNL scores were significantly lower than the baseline values at the first month (p=0.0001). Although there was a slight increase compared to the first month, one-year follow-up values of the same parameters were still significantly lower than the baseline (p=0.0001) (Table 1, Figure 1 and Figure 2).
At the end of the first month, there was a significant correlation between the differences in the variation percentages of SL, J, and FD values (p=0.0001 for SL and J, p=0.037 for FD). HNL values did not show any significant correlation with other parameters (p>0.05). At one-year follow-up, the variation percentage of SL had a positive correlation with J values (p=0.0001), and the variation percentage of J correlated positively with SL and FD values (p=0.004 for SL and p=0.039 for FD).
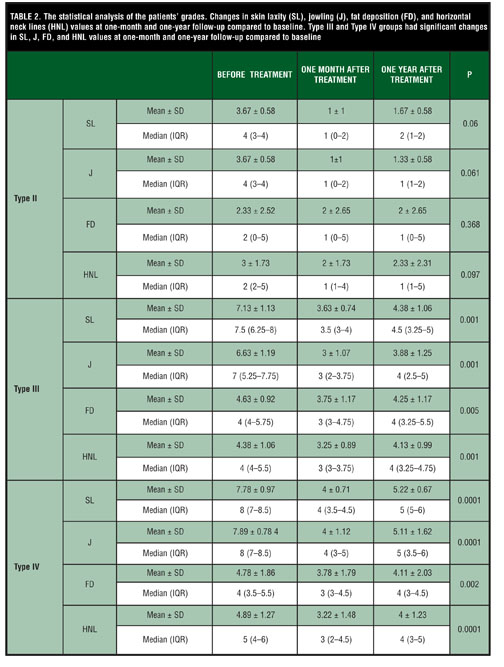
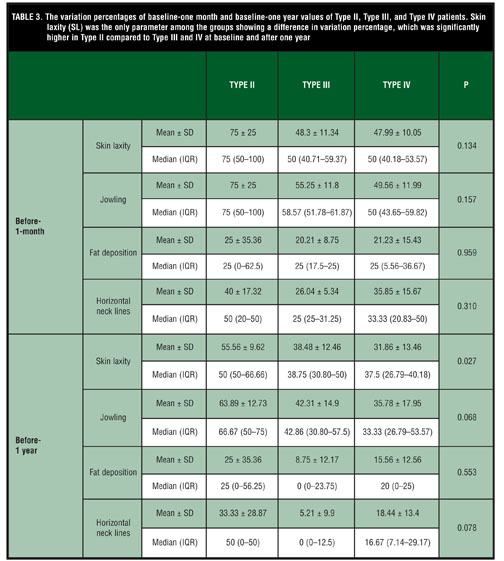
The statistical analysis of the patients’ grades showed that Type III and Type IV groups had significant changes in SL, J, FD, and HNL values at one-month and one-year follow-up compared to baseline (p<0.05) (Table 2). The variation percentages of baseline and first month values of Type II, Type III, and Type IV did not show any significant difference between the groups (p>0.05), whereas there was a significant difference at SL values among the groups at baseline and after one year, as SL was the only parameter showing a difference in variation percentage, which was significantly higher in Type II compared to Type III and IV (p=0.027) (Table 3).
No serious or persistent complications, such as prolonged erythema, hypopigmentation, and scarring, developed in any of the patients. Short-lasting adverse effects included erythema (up to 14 days), edema (up to 3 days), epidermal bronzing, crusting, exfoliation, and infection. The most common adverse reaction was postinflammatory hyperpigmentation, which occurred in five patients (25%) with Fitzpatrick skin types III and IV. Postinflammatory hyperpigmentation resolved within three months with topical hydroquinone 4% cream and daily application of broad-spectrum sunscreen with SPF 50. One of the 20 (5%) patients developed Staphylococcus aureus infection and one (5%) patient developed Candida albicans infection, both of which were noticed at the seventh day follow-up visit. They were treated with appropriate systemic medications, and in order to avoid scar formation, the infected areas were treated with pulsed dye laser (PDL) immediately after epithelization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
The pathophysiology of the aging neck involves multiple factors that may effect the results of the recommended treatment. Photodamage, gravity, changes in weight, and fat tissue accumulation may all contribute to neck aging. The skin may develop laxity due to alterations in the connective tissue matrix combined with the downward vector effect of gravity; or the occurrence of the characteristic platysmal bands due to the hypertrophy of the platysma; or fat accumulation and fat repositioning in the subcutaneous and subplatysmal planes leading to localized adiposity. Ultraviolet exposure can also create vascular changes leading to Poikiloderma of Civatte. Overall, the patient can display one or more of these features. Therefore, it is very critical to evaluate the main pathological process in each patient before planning the treatment in order to achieve optimal improvement 4.
The clinical results of fractionated ablative laser resurfacing are often found to approach those of full field CO2 resurfacing, which is the gold standard of laser rejuvenation, with fewer side effects and shorter downtime. The improvement in quality, texture, elasticity, and turgor of the skin, secondary to full field CO2 laser surfacing, is explained by the immediate shrinkage of the collagen, and also by neocollagenesis and neoelastogenesis starting within weeks of treatment.[9] In a recent study by Orringer et al,[10] comparing the molecular changes after a single treatment of fractionated or fully ablative CO2 laser resurfacing, both systems were shown to induce significant dermal remodeling and collagen induction, although the effects differed in magnitude and duration. Fractionated ablative laser resurfacing resulted in 40- to 50-percent collagen induction that was pronounced as that induced by fully ablative laser. Tierney and Hanke[11] demonstrated a 63-percent improvement in skin texture, a 57-percent mean improvement in skin tightening, and a 51.4-percent improvement in skin rhytides at two months post treatment by using a fractionated CO2 laser for neck rejuvenation. Similarly, our study clearly shows that fractional CO2 laser is an effective treatment for neck aging, even after one session. All patients showed significant improvement in SL, J, FD, and HNL. A better skin texture and color was also observed with the treatment. The clinical outcome at the first month was maintained, but to a lesser degree at the end of one year.
It is known that, after the skin is ablated with fractional CO2 laser, there is a bimodal effect, first from immediate collagen contraction and second from persistent collagen remodeling after 3 to 6 months.[6] The immediate contraction and shrinkage of the collagen is most likely to cause the early skin tightening and prominent improvements of the parameters in our cases at one-month follow-up. However, after collagen remodeling at the one-year follow-up, the patients continued to show a better outcome compared to the baseline. Ortiz et al[12] also reported the long-term outcomes of 10 patients previously treated with fractional CO2 resurfacing. They demonstrated that the subjects maintained 74 percent of the overall improvement at long-term visits compared with three-month follow-up visits.
The most impressive finding of this study was the significant and consistent effect of the treatment on SL values. The authors believe that the dramatic improvement of SL leads to skin tightening and causes positive effects on J and FD, both in early and long-term periods, regarding the significant correlation observed in the study. Moreover, the SL value was the only parameter showing significant alteration according to the severity of the neck aging. Thus, patients who had moderate skin laxity and moderate jowling (Type II) showed a better response in skin tightening.
The procedure had minimal downtime and side effects while providing reliable and predictable results. Although the overall complication rate was 35 percent, they were all transient. However, even the experienced laser surgeons should be cautious when treating the neck with ablative lasers, as the neck is prone to develop hypertrophic scarring after thermal injury.[13–15] The fewer pilosebaceous units and more limited cutaneous vasculature on the neck, together with excessive laser energy settings and overlapping, as well as postoperative wound infections are implicated to be the possible explanations of this phenomenon.[13–15] Therefore, it is crucial to apply conservative energy settings and to follow up patients frequently after the procedure in order to prevent, realize, and treat any signs of infection or focal areas of persistent erythema, which are the first signs of hypertrophic scarring. PDL therapy is one of the early treatment options for the prevention of hypertrophic scarring after fractional laser therapy.[15] The authors performed PDL to the limited areas of infection in addition to the appropriate antimicrobial treatment in two of their patients.
In conclusion, the results of this study confirm that fractional CO2 neck rejuvenation is an effective treatment option with long-term efficacy for patients who mainly have skin laxity and jowling together with skin surface pigmentation. Obviously, fat deposition is not directly affected from the treatment; however, the skin tightening effect provides a better appearance in fat tissue. Although there exists an improvement in horizontal neck lines, this is variable and unpredictable. Patients with moderate aging are more likely to display a better outcome. The clinical improvement is maintained at one year, although the results are not as remarkable as those seen at one-month follow-up. Additional treatment sessions would possibly provide an enhancement in the clinical results with longer efficacy.
References
1. Caplin DA, Perlyn CA. Rejuvenation of the aging neck: current principles, techniques, and newer modifications. Facial Plast Surg Clin North Am. 2009;17:589–601.
2. Collawn SS. Skin tightening with fractional lasers, radiofrequency, Smartlipo. Ann Plast Surg. 2010;64:526–529.
3. Lee HS, Jang WS, Cha YJ, et al. Multiple pass ultrasound tightening of skin laxity of the lower face and neck. Dermatol Surg. 2012;38:20–27.
4. Brandt F, Boker A, Moody BR. Neck treatment. In: Carruthers A, Carruthers J, eds. Procedures in Cosmetic Dermatology– Botulinum Toxin. China: Elsevier Saunders; 2005:71–79.
5. Alexiades-Armenakas M. Combination laser-assisted liposuction and minimally invasive skin tightening with temperature feedback for treatment of the submentum and neck. Dermatol Surg. 2012;38:871–881.
6. Tierney EP, Eisen RF, Hanke CW. Fractionated CO2 laser skin rejuvenation. Dermatol Ther. 2011;24:41–53.
7. Alexiades-Armenakas M, Sarnoff D, Gotkin R, Sadick N. Multi-center clinical study and review of fractional ablative CO2 laser resurfacing for the treatment of rhytides, photoaging, scars and striae. J Drugs Dermatol. 2011;10:352–362.
8. Baker DC. Lateral SMASectomy, plication and short scar facelifts: indications and techniques. Clin Plast Surg. 2008;35:533–550.
9. Rosenberg GJ, Brito MA Jr, Aportella R, Kapoor S. Long-term histologic effects of the CO2 laser. Plast Reconstr Surg. 1999;104:2239–2244.
10. Orringer JS, Sachs DL, Shao Y, et al. Direct quantitative comparison of molecular responses in photodamaged human skin to fractionated and fully ablative carbon dioxide laser resurfacing. Dermatol Surg. 2012;38:1668–1677.
11. Tierney EP, Hanke CW. Ablative fractionated CO2, laser resurfacing for the neck: prospective study and review of the literature. J Drugs Dermatol. 2009;8:723–731.
12. Ortiz AE, Tremaine AM, Zachary CB. Long-term efficacy of a fractional resurfacing device. Lasers Surg Med. 2010;42:168–170.
13. Avram MM, Tope WD, Yu T, et al. Hypertrophic scarring of the neck following ablative fractional carbon dioxide laser resurfacing. Lasers Surg Med. 2009;41:185–188.
14. Hunzeker CM, Weiss ET, Geronemus RG. Fractionated CO2 laser resurfacing: our experience with more than 2000 treatments. Aesthet Surg J. 2009;29:317–322.
15. Metelitsa AI, Alster TS. Fractionated laser skin resurfacing treatment complications: a review. Dermatol Surg. 2010;36:299–306.