
Anthony J. Chiaravalloti, MD; Jeffrey R. LaDuca, PhD, MD
Anthony J. Chiaravalloti, MD, is from SUNY Upstate Medical University, Syracuse, New York. Jeffrey R. LaDuca, PhD, MD, is from Reflections Dermatology and Psoriasis Center, Auburn, New York.
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Objective: Previous studies have shown that dermatologists detect thinner melanomas than both non-dermatologists and patients in high incidence areas. The authors report depths of melanomas in a central New York practice where the incidence is low, hypothesizing that incidental melanomas detected by a dermatologist will be thinner than melanomas that are part of the chief complaint. Design: A retrospective chart review examining melanoma depth to determine the importance of universal full skin exams. Setting: Private dermatology clinic in Auburn, New York, employing one board-certified dermatologist and two physician extenders. Participants: Men and women who attended the clinic between 2003 and 2013 who had 235 biopsy-proven melanomas. Total patient visits in this time period was 50,699. Measurements: Office notes were reviewed to determine the chief complaint, patient demographics, and depth of the tumor. The authors noted if the melanoma was discovered by the patient, a referring physician, dermatology physician extender, or the dermatologist. Results: More than 45 percent of melanomas were an incidental finding on full skin exam. The dermatologist detected statistically thinner melanomas than melanomas that presented as the chief complaint. The dermatologist tended to detect thinner melanomas than referring physicians and patients. Conclusion: A significant portion of melanomas are incidentally found on full skin exam, and thinner melanomas are detected by dermatologists. Universal skin cancer screening takes little additional time, and appropriate use of physician extenders can greatly increase access to dermatological care. Full skin exams increase melanoma detection, decreases overall thickness at diagnosis, and decreases patient morbidity and mortality. (J Clin Aesthet Dermatol. 2014;7(8):18–22.)
Melanoma is the most deadly type of skin cancer with limited treatment for deep tumors. The average age adjusted melanoma death was 2.73 per 100,000 in the United States between 2006 and 2010.[1] Thus, early detection of melanoma offers the best hope for a cure. Cutaneous melanoma presents a unique opportunity for intervention compared to other malignancies, as screening is simple, noninvasive, and takes little time. Clinical full skin exams have been shown to decrease the number of deep melanomas,[2] which is important because the depth of invasion for malignant melanoma is the most important prognostic factor. However, even with the availability of such an easy screening test, the guidelines of when and whom to screen are unclear.[3] The effect of screening on patient mortality has not been studied in a randomized trial, and formal guidelines are lacking. Previous studies have attempted to determine who detects melanomas and how they present in their clinics.[2,4–6] Several of these studies were performed in areas of higher incidence of melanoma, such as Australia2 and Florida.[6] The aim of this study is to report the percentage of the authors’ patients incidentally found to have melanoma as part of a full skin exam and to compare the depth of invasion with patients whose melanoma was related to their chief complaint. The authors compare their data from a private practice near Syracuse, New York, which has a relatively low incidence of melanoma in the United States,1 to some of the previously reported studies and make recommendations for future screening.
Methods
The authors performed a retrospective chart review at a private dermatology office in a suburb of Syracuse, New York, between 2003 and 2013. During this time period, 50,699 patients were seen at this practice. At this practice, all patients regardless of their age, history, and chief complaint are encouraged to receive a full skin exam. A full skin exam consists of a head-to-toe exam with dermoscopy. The scalp is examined by pulling back hair. Oral mucosal is examined. The genitals are not routinely examined unless the patient has a specific concern. The practice consists of one board-certified dermatologist and two physician extenders. The chart review was completed by filtering the diagnosis code for malignant melanoma. This computerized list was then cross referenced against a written record of biopsy results for the practice. Each patient used in the analysis had biopsy-proven malignant melanoma diagnosed by a dermatopathologist. The authors included melanoma in situ, lentigo maligna, and invasive melanomas in their analysis. Depth of invasion for invasive melanomas was calculated using the depth measured in millimeters as provided by the final dermatopathology report upon full excision of the melanoma. Melanoma in situ and lentigo maligna melanomas were measured as 0.0mm for the analysis. Patients referred to the practice with previously diagnosed, biopsy-proven melanoma were not included. Office notes were reviewed to determine the chief complaint of the visit when the melanoma was diagnosed, patient demographics, and depth of the tumor. The authors also recorded if the lesion was discovered by the patient, a referring physician, dermatology physician extender, or the dermatologist. The Mann-Whitney U test was used to determine p values for data sets. Statistical significance was set at p<0.05.
Results
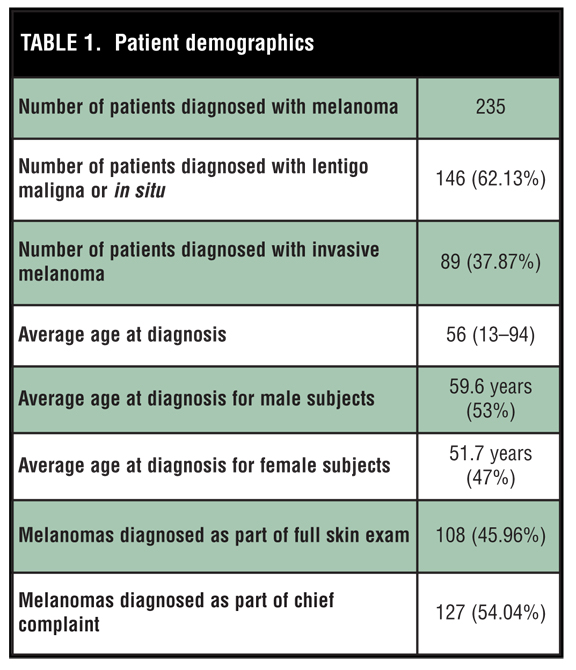
Two hundred and thirty-five patients with melanoma were identified and included in this study. Melanoma in situ and lentigo maligna accounted for 62.13 percent of the melanomas. The remaining 37.87 percent were invasive melanomas. The average age of the group was 56 years with average for males and females being 59.6 and 51.7 years, respectively. The age range studied was 13 to 94 years. Males accounted for 53 percent of the group. Of the melanomas diagnosed during this period, 54.04 percent of the cases were related to the chief complaint at the time of visit, while 45.96 percent were unknown to the patient and detected as the result of a full skin examination by either the dermatologist or dermatology physician extender (Table 1).
{kind=link}
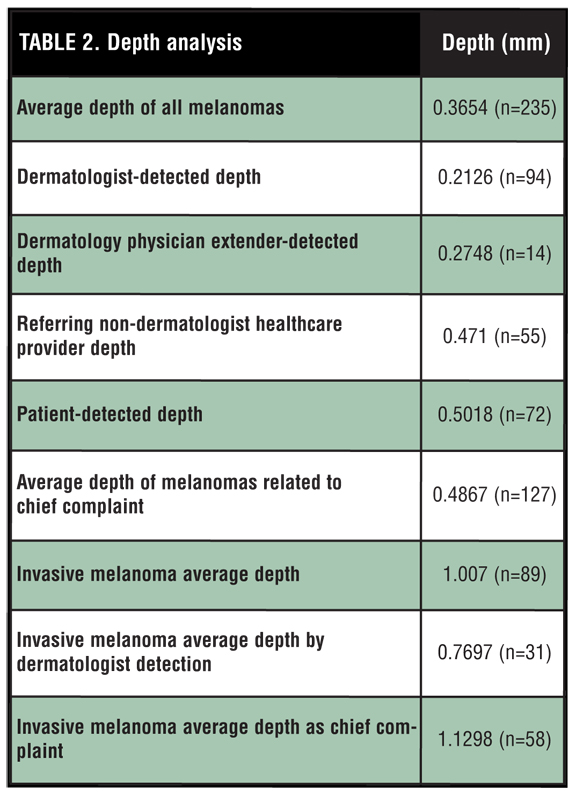
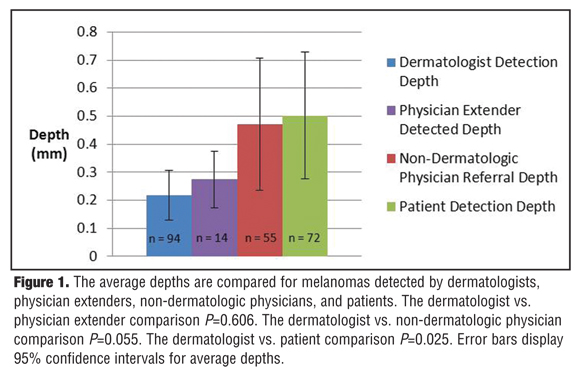
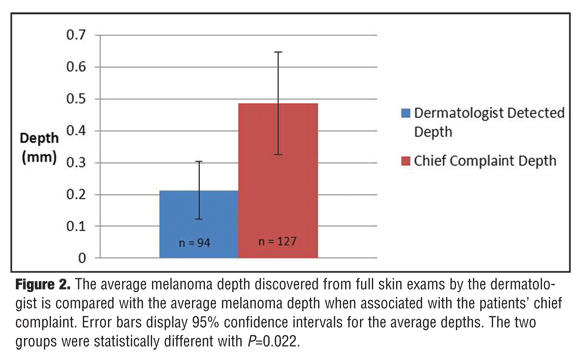
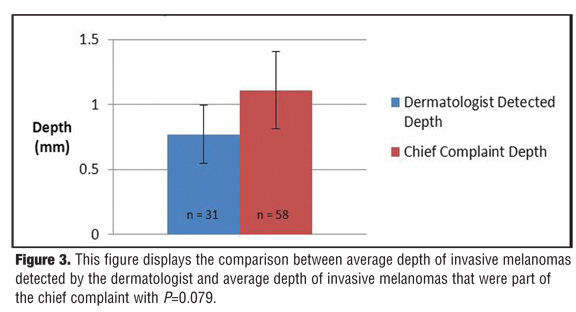
Table 2 illustrates the depth analysis of melanomas diagnosed. The dermatologist saw 87.3 percent of the cases and the physician extenders saw 12.7 percent of the cases. When the dermatologist made the diagnosis of incidental melanoma, the average depth of invasion was thinnest at 0.2126mm. When the dermatology physician extender made the diagnosis as part of their skin examination, the depth was 0.2748mm. Non-dermatologist primary care providers referred patients to the practice with melanomas averaging 0.471mm. And when patients detected their own melanomas, the depths were the thickest at 0.5018mm on average (Figure 1). The average dermatologist-detected depth was statistically thinner than melanomas that presented as the patients’ chief complaint (Figure 2). The average depth of all invasive melanomas was 1.007mm. The dermatologist detected incidental invasive melanomas at an average depth of 0.7687mm. The average depth for invasive melanomas that presented as the patients’ chief complaint was thicker at 1.1298mm (Figure 3).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
The depth of the melanoma at diagnosis is the most important prognostic factor. The five-year survival rate for melanomas in situ is 99.9 percent while melanomas 1.01 to 2.0mm in depth have a five-year survival of 45 to 79 percent.[7] The standard of care calls for excision of deeper tumors with up to 2cm margins.[8] Additionally, melanomas over 1mm in depth have an indication for lymph node evaluations. Thus, detection of melanomas when thinner offers less morbidity and mortality.
In this study, nearly 46 percent of the melanomas diagnosed at this clinic were unknown to the patient and not related to their chief complaint. When comparing the overall depth of invasion of these melanomas, the dermatologist-diagnosed melanomas were thinner (0.2126mm) compared with tumors recognized by the patient or referring primary care providers (0.4867mm) (p=0.022). The results from this study are consistent with previous studies comparing depths of melanomas as a result of screening versus the chief complaint.[4,6] Two studies found that 39.5 percent[4] and 56.7 percent6 of melanomas were found incidentally as the result of a dermatologist’s full skin exam. The authors’ average melanoma depth from full skin exams was 0.2126mm, which was similar to previously reported depths of 0.21mm[4] and 0.16mm.[6] All three studies come to the same conclusion that dermatologist-detected melanomas are thinner than melanomas that are part of the chief complaint. This fact should correlate with a mortality benefit.
The data from this study show that 62.13 percent of melanomas were in situ or lentigo maligna type. When excluding these tumors, the authors found that dermatologist-detected invasive melanomas tended to be thinner as well. The average depth of all invasive melanomas included was 1.007mm. However, when split into subgroups, the average depth of invasive melanomas discovered on full skin exam (0.7697mm) was less than the average depth of invasive melanomas that were the patient’s chief complaint (1.1298mm). Although this did not achieve statistical significance (p=0.079), it may still suggest a trend that dermatologists detect thinner invasive melanomas as well as melanomas in general.
The authors compared the melanoma depths when detected by the dermatologist, physician extenders, primary care providers, and patients. The melanomas detected by the dermatologist were thinnest at 0.2127mm followed by the dermatology physician extenders at 0.2748mm (p=0.606). The primary care provider-detected melanomas averaged 0.4710mm (p=0.055) while patient-detected melanomas averaged 0.5018mm (p=0.025). Previous studies have showed patient-detected melanoma depths between 0.26mm4 and 0.40mm.[6] In another study, non-dermatologist physicians discovered melanomas with an average depth of 0.68mm.[5] Although the dermatologist versus primary care referral subgroups were not statistically significant,[5] the authors’ numbers still suggest that dermatologists detect thinner melanomas compared with patients and non-dermatologist physicians. The dermatologists detected more melanomas (94) than any other group in this study again supporting the importance of melanoma screening by a dermatologist. This trend is furthered by previous studies showing melanomas detected by dermatologists had higher survival rates at six months, two years, and five years compared with melanomas detected by non-dermatologists.[9]
A full skin exam in the last three years was shown to be associated with increased likelihood of thin (<0.75mm) melanoma and a decreased risk of thick (0.75mm or greater) melanomas[2]; however, only 30 percent of dermatologists and 31 percent of primary care physicians screen all patients for skin cancer.[10] When examining high-risk patients, 70 percent of dermatologists and 31 percent of primary care providers screen.[10] Lack of time was cited as the number one reason why a full exam was not performed.[10] Time is an important consideration for all physicians, especially for dermatologists. Nationwide shortages exist with a national average wait time of 33 days for a new patient to be seen by a dermatologist.[11] It is even more difficult to be seen by a dermatologist in the authors’ geographic region where the average wait is 47.9 days.[12]
It has been estimated that a full skin exam takes only 70 seconds without dermoscopy and six minutes with dermoscopy.[13] Only 20 percent of dermatologists reported regularly using dermoscopy for skin exams,[14] meaning for the majority of these providers, a full skin exam would take a little over a minute. One of the ways that this private practice attempts to create more time for full skin exams is through the use of physician extenders. The utilization of physician extenders is effective in increasing access to care as they have been shown to be able to see new patients on an average of 17 days sooner than the dermatologist in a practice.[12] Physician extenders in our practice are used for follow-up visits, prescription refills, and urgent appointments. This frees the board-certified dermatologist to focus on patients with a history of malignancy and complex dermatological conditions as well as patients on complicated medications. Properly trained physician extenders, under close supervision of a board-certified dermatologist, can make invaluable contributions to a dermatology practice. The authors’ physician extenders accounted for the detection of 12.7 percent of the melanomas included in this study. Their average detection depth was thinner than patient- and referring physician- detected depths. Ideally, well trained dermatology physician extenders would detect melanomas at a depth similar to the dermatologist. In this study, the depths by the dermatologist and the physician extenders were not statistically different (p=0.606).
This model of universal screening has been very successful in the authors’ practice and they recommend it as a way to increase the percentage of patients who receive a full skin exam. This policy found incidental melanomas in a teenager who presented for an acne recheck and a middle-aged woman who presented for a cosmetic consult. These cases highlight the unpredictability of melanoma and importance of screening. For practices that cannot comply with full exams for all, it has been previously recommended that anyone over 50 years of age with a personal or family history of skin cancer be screened.[4] The authors advocate that clinical judgment be used to screen people with significant risk factors annually. Important risk factors include Fitzpatrick skin types I and II, blond hair, blue eyes, personal or family history of melanoma, many nevi, atypical nevi, history of tanning booth use, and history of blistering sunburns. Regardless of risk factors, the authors recommend that all new patients receive a full skin exam.
One limitation of this study is that this is a retrospective study on tumor depth and does not examine mortality. The authors recommendations are based on previous evidence that tumor thickness corresponds to mortality. The ideal study to examine the mortality benefit of screening would be a randomized controlled trial with mortality as the primary outcome. This has been suggested before, but still appears to be cost-prohibitive.[2] Another limitation of this study is that the authors could not measure the sensitivities of their exams. It is possible that melanomas are initially missed and found on subsequent exams. It is encouraging that the depths on diagnosis were still very shallow by physician extenders and the dermatologist, making this most likely a rare event.
Conclusion
The authors have shown that dermatologists detect a significant amount of melanomas in their practice from full skin exams. Dermatologists detect thinner melanomas at diagnosis compared with patient detection and primary care referrals, which directly correlates with a better prognosis. The authors advocate for full skin exams for all patients who come to a dermatology clinic. Their data shows that there is a benefit of full skin exams even in Syracuse, New York, where the incidence of melanoma is lower than other parts of the United States. The use of physician extenders can greatly increase the access to care and reduce some of the patient burden for dermatologists. For clinics that absolutely cannot give full skin exams to everyone, the authors recommend full exams for all new patients with subsequent screenings based on clinical judgment of important risk factors previously mentioned. Self-skin exams should be encouraged among all patients. The authors urge reassessment of the literature to examine studies such as this one that support dermatological screening to decrease tumor thickness with the ultimate goal of creating formal melanoma screening guidelines.
References
1. SEER Cancer Statistics Review 1975-2010. Melanoma of the Skin. April 2013. http://seer.cancer.gov/csr/1975_2010/results_ merged/sect_16_melanoma_skin.pdf. Accessed on June 20, 2013.
2. Aitken JF, Elwood M, Baade PD, et al. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010;126(2):450–458.
3. Counseling to prevent skin cancer: recommendations and rationale of the U.S. Preventive Services Task Force. MMWR Recomm Rep. 2003;52(RR–15):13–17.
4. Mcguire ST, Secrest AM, Andrulonis R, Ferris LK. Surveillance of patients for early detection of melanoma: patterns in dermatologist vs patient discovery. Arch Dermatol. 2011;147(6):673–678.
5. Cherian P, Tait CP. Melanoma in private practice: do dermatologists make a difference? Australas J Dermatol. 2009;50(4):257–260.
6. Kantor J, Kantor DE. Routine dermatologist-performed full-body skin examination and early melanoma detection. Arch Dermatol. 2009;145(8):873–876.
7. Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27(36):6199–6206.
8. Bichakjian CK, Halpern AC, Johnson TM, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2011;65(5):1032–1047.
9. Pennie ML, Soon SL, Risser JB, et al. Melanoma outcomes for Medicare patients: association of stage and survival with detection by a dermatologist vs. nonderm. Arch Dermatol. 2007;143(4):488–494.
10. Federman DG, Kravetz JD, Kirsner RS. Skin cancer screening by dermatologists: prevalence and barriers. J Am Acad Dermatol. 2002;46(5):710–714.
11. Kimball AB, Resneck JS. The US dermatology workforce: a specialty remains in shortage. J Am Acad Dermatol. 2008;59(5):741–745.
12. Tsang MW, Resneck JS. Even patients with changing moles face long dermatology appointment wait-times: a study of simulated patient calls to dermatologists. J Am Acad Dermatol. 2006;55(1):54–58.
13. Hantirah SA, Yentzer BA, Karve SJ, et al. Estimating the time required for a complete skin examination. J Am Acad Dermatol. 2010;62(5):886–888.
14. Reyes ortiz CA, Freeman JL, Kuo YF, Goodwin JS. The influence of marital status on stage at diagnosis and survival of older persons with melanoma. J Gerontol A Biol Sci Med Sci. 2007;62(8):892–898.